

서 론
백내장 수술 기술의 발전과 인공 수정체의 발달로 오늘 날 백내장 수술은 단순히 백내장만을 제거하는 것이 아니라, 굴절 이상 및 노안의 교정까지 추구하고 있다. 각막이 가진 양의 구면 수차를 교정하기 위해 음의 구면 수차를 가진 다양한 비구면 인공수정체가 개발되어[1,2], 수술 후 고위 수차를 줄이고[3], 특히 동공이 확장되어 있을 때[4] 대비 감도와 시력을 향상시키는 것이[5,6], 백내장 수술의 목표 중 하나로 자리잡았다.
ARTIS® PL E (Cristalens Industrie, Lannion, France)는 기존에 국내에서도 널리 이용된 일체형 비구면 인공수정체로 -0.10 μm의 음의 구면수차값을 가지고 있으며 4개의 고리 모양의 지지부와 6 mm 지름의 광학부로 구성되어 있다[7]. Primus-HD® (Ophthalmo Pro GmbH, Sankt Ingbert, Germany)는 A1-UV (Eyebright Medical Technology Inc, Beijing, China)를 Prosert® (Ophthalmo Pro GmbH) 인공수정체 주입기와 결합시켜 유럽에서 새롭게 출시된 preloaded 인공수정체이다. Primus-HD®는 -0.20 μm의 더 큰 음의 구면 수차를 갖는 소수성 아크릴 비구면 인공수정체이다[8]. 두 인공수정체 모두 2.0 mm 크기의 각막 절개를 통해 이식할 수 있는 preloaded 인공수정체이다(Table 1).
인공수정체는 한번 체내에 삽입하면 대개의 경우 교체하지 않고 평생 보유하게 되는 만큼 백내장 수술 후 인공수정체의 효과, 안전성, 그리고 장기적인 안정성에 대한 관심이 대두되고 있다. A1-UV 인공수정체는 기존의 비구면 인공수정체와 비교하여 수술 후 교정시력과 나안시력은 비슷하지만 인공수정체의 반짝임 변성(glistening) 발생률은 낮다는 연구들이 보고되었다[9,10].
그러나 현재까지 국내외에 Primus-HD® preloaded 인공수정체의 임상적 결과를 보여주는 연구는 없었으며, 따라서 본 연구에서는 기존에 국내에서 널리 사용되던 비구면 preloaded 인공수정체인 ARTIS® PL E와 비교하여 이 새로운 인공수정체의 임상 결과를 평가하고자 한다.
대상과 방법
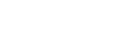
이 연구는 단일센터에서 진행된 후향적 연구로 연세대학교 의과대학 부속 세브란스병원 임상시험심사위원회(Institutional Review Board)와 윤리위원회의 심사를 승인(승인 번호: 4-2023-0051) 받았으며, 헬싱키 선언을 준수하여 수행되었다. 비식별화된 환자 데이터를 사용한 후향적 연구로, 연구 참여에 대한 환자 동의는 면제되었다. 2021년 4월 19일부터 2022년 11월 30일까지 연세대학교 의과대학 부속 세브란스병원에서 단일 술자(IJ)에 의해 ARTIS® PL E (A군) 또는 Primus-HD® (B군) 인공수정체를 이용해 백내장 수술을 받은 환자들이 연구에 포함되었다.
50세 이상의 노년성 백내장[11] 환자들이 연구에 포함되었다. (1) 안구 수술 또는 외상(n = 13)의 병력, (2) 녹내장(n = 13), 황반질환(n = 49), 안축장 26 mm 초과 또는 22 mm 미만의 심한 근시와 원시(n = 19), 각막 혼탁(n = 8), 1,500 미만의 낮은 내피 세포 수 또는 심한 구타타(n = 19), 거짓비늘증후군(n = 6), 포도막염(n = 1), 성상유리체증(n = 1), 약시(n = 2) 등 수술 후 시력예후에 영향을 줄 수 있는 안과적 과거력, 그리고 (3) 백색 백내장(n = 6)이 있는 눈은 연구에서 제외되었다(Fig. 1).
수술 전 평가
수술 전 검사는 양 군에서 모두 동일하게 시행되었으며 세극등 및 안압 검사, 나안시력, 최대교정시력, 현성굴절검사, 안저검사, 각막내피세포검사, 각막지형도검사(Pentacam HR; Oculus, Wetzlar, Germany) 및 안구수차검사(Tracey Technologies Corp., Houston, TX, USA)가 이에 포함되었다. 고위수차의 root mean square 값과 트레포일 수차, 코마 수차, 구면 수차는 4 mm 동공에서 측정되었다[12]. 인공수정체 도수는 IOL Master-700 (Carl Zeiss Meditec, Oberkochen, Germany)를 이용하여 측정하고 목표 디옵터는 SRK/T, Barrett Universal II 및 Haigis 공식을 사용하여 계산하였다. SRK/T 공식으로 계산한 목표 디옵터를 기준으로 근시가 -0.25 D에 가장 근접한 IOL을 택하였다.
수술 후 평가
수술 후 검사는 수술 후 1일, 1주, 1개월, 그리고 3개월째에 시행되었으며, 나안 원거리(3 m) 시력, 안압, 세극등검사, 자동각막 굴절검사를 포함하였다. 수술 후 1개월 및 수술 후 3개월차 검사에는 나안 중간거리 시력(66 cm)과 근거리 시력(33 cm), 현성 굴절법을 이용한 최대 교정 원거리 시력, iTrace® (Tracey Technologies Corp., Houston, TX, USA)를 이용한 각막수차측정 및 각막내피세포수 검사가 포함되었다. 수술전에 계산된 목표 디옵터와 수술 후 3개월째에 굴절률을 비교하여 평균오차와 평균 절대오차를 계산하였으며, 평균 오차는 수술 후 3개월째 굴절률에서 각 공식으로 계산한 목표 디옵터를 뺀 값의 평균으로, 평균 절대오차는 수술 후 3개월째 굴절률에서 각 공식으로 계산한 목표 디옵터를 뺀 값의 절대값의 평균으로 계산하였다.
결 과
A군의 43명 69안, B군의 19명 36안을 대상으로 하였다. 수술 중 혹은 수술 후 합병증은 두 그룹 모두에서 관찰되지 않았다. A군의 평균 연령은 73.29 ± 8.03세였으며 B군의 평균 연령은 74.83 ± 5.43세로 양 군 간 유의한 차이가 없었다(Table 2). 연령, 성별, 수술 전 나안 원거리 시력, 최대교정 시력, 구면 렌즈 대응치, 안축장, 전방 깊이(Table 2), 고위수차(Table 3) 또한 두 군 간에 유의한 차이가 없었다.
수술 후 3개월 시점에서 양 군의 임상적 결과는 Table 4에 나타나 있다. 수술 후 3개월 시점에 나안 원거리 시력(A군과 B군에서 각각 0.15 ± 0.17 및 0.17 ± 0.18, p = 0.60), 최대 교정 원거리 시력(A군과 B군에서 각각 0.03 ± 0.06 및 0.02 ± 0.05, p = 0.75), 나안 중간 거리 및 근거리 시력에는 두 군 간의 유의미한 차이가 없었다(Table 4). 수술 후 굴절력(A군과 B군에서 각각 -0.16 ± 0.85 D 및 -0.47 ± 0.66 D, p = 0.10) 및 난시 굴절값(A군과 B군에서 각각 -0.43 ± 0.45 D 및 -0.43 ± 0.56 D, p = 0.96) 또한 두 군 간의 차이가 없었다. A군에서 수술 후 1개월에 굴절률과 비교하여 수술 후 3개월에는 0.03 ± 0.34 D만큼 원시 방향으로 굴절률이 이동한 반면, B군에서는 3개월차에 -0.07 ± 0.30 D만큼 근시 방향으로 굴절률이 이동한 것을 확인할 수 있었으나 유의미한 차이는 없었다(p = 0.19) (Table 4).
수술 후 3개월 차에 SRK/T 공식의 평균오차(A군과 B군에서 각각 0.26 ± 0.53 및 -0.08 ±0.42, p < 0.01) 및 Barrett Universal II 공식의 평균오차(A군과 B군에서 각각 0.53 ±0.53 및 -0.03 ±0.33, p < 0.01)는 A군에 비해 B군에서 유의하게 작았다. Haigis 공식에 대한 평균오차는 두 그룹 간에 유의미한 차이가 없었다. 반면, 평균 절대오차의 경우 Barrett Universal II (수술 후 3개월째에 A군과 B군에서 각각 0.61 ± 0.42 D 및 0.28 ± 0.17 D, p < 0.01)와 Haigis (수술 후 3개월째에 A군과 B군에서 각각 0.51 ± 0.38 D 및 0.33 ± 0.23 D, p = 0.01) 모두 A군에 비해 B군에서 유의미하게 낮았다(Table 4).
B군 내에서는 수술 후 3개월째에 Barrett Universal II 공식이 SRK/T 공식보다 예측력이 유의미하게 더 높았다(Barrett Universal II 및 SRK/T 공식의 절대 오차값 각각 0.28 ± 0.17 및 0.36 ± 0.22, p = 0.02). Haigis 공식의 예측력은 SRK/T (p = 0.67) 및 Barrett Universal II (p = 0.11) 공식과 유사했다(Table 4).
연구에 포함된 모든 환자의 모든 안에서 수술 전, 수술 후 1개월, 수술 후 3개월 고위수차 측정을 시행하였다. 수술 후 3개월 시점에서 안구 전체 수차, 구면수차 및 코마수차는 두 군 간에 유의한 차이가 없었다(Table 3). 안구 내 구면수차의 교정량(수술 후 안구 내 구면수차와 수술 전 안구 내 구면수차의 차이)은 A군에서 0.00 ± 0.45, B군에서 -0.10 ± 0.45로 나타났으나 두 군 간에 유의미한 차이는 없었다(p = 0.37).
고 찰
중국에서 진행된 몇몇 기존 연구에서는 A1-UV 인공수정체가 근거리 및 원거리 나안 시력, 최대 교정시력, 대비 민감도, 주관적 만족도 측면에서 기존에 안정성이 검증된타 비구면 인공수정체와 차이가 없음을 입증했다[9,10,13]. 그러나 현재까지 국내외에서 Primus-HD® preloaded 인공수 정체의 임상 결과를 다른 인공수정체와 비교한 국내 및 국제적 보고는 없었다.
본 연구에서 Primus-HD® 인공수정체를 이용한 백내장 수술이 기존에 효능과 안전성이 확립된 비구면 단초점 인공수정체인[14] ARTIS® PL E를 이용한 백내장 수술과 유사한 결과를 보여주었다. 두 인공수정체 모두 preloaded 인공수정체로, 수술 중 인공수정체 삽입에 소요되는 시간을 단축시키고, 인공수정체 장착 중 발생 가능한 광학부 긁힘 및 오염을 방지하는 것으로 알려져 있다[15,16].
예측성 측면에서는 Barrett Universal II와 Haigis 공식 모두 평균 절대오차 값이 A군에 비해 B군에서 유의미하게 낮아 우수한 예측성을 보였다. ARTIS® PL E 인공수정체를 삽입한 백내장 수술에서는 SRK/T, Barrett Universal II 및 Haigis 공식으로 계산한 목표 디옵터에 비해 실제 수술 후 굴절률이 원시에 가깝게 나타난 반면, Primus-HD® 인공수정체를 이용한 백내장 수술을 받은 환자는 세 가지 공식으로 계산된 목표 디옵터와 비교하여 실제 굴절률은 더 근시에 가깝게 나타났다.
인공수정체 광학부의 전후방 움직임은 백내장 수술 후 굴절 안정성에 중요한 요소이며, 이로 인해 백내장 수술 후 굴절력이 근시 혹은 원시로 이행할 수 있다[17,18]. 이 연구에서 수술 후 3개월 평가에서 ARTIS® PL E 및 Primus-HD® 인공수정체 모두 유의미한 굴절력의 변화가 관찰되지 않았다.
비구면 인공수정체는 수술 후 안구 내 구면 수차를 음의 값으로 만들어 각막의 양의 구면수차를 상쇄함으로써 안구 전체 구면수차를 0에 가깝게 유지하도록 설계되어 있다[2,19]. Primus-HD® 인공수정체의 자체적인 구면수차 값은 -0.20 μm로 ARTIS® PL E 인공수정체 -0.10 μm에 비해 크며, 본 연구에서도 백내장 수술 전 후 안구 내 구면수차의 교정량은 A군에서 0.00 ± 0.45, B군에서 -0.10 ± 0.45 (p = 0.37)로 Primus-HD®로 인한 안구 내 구면수차 교정량이 -0.10 μm 더 큰 것을 확인할 수 있었으나, 유의미한 차이는 없었다.
한편, 본 연구에서는 A, B군 모두 수술 후 각막 구면수차의 값이 수술전에 비해 감소한 것으로 나타났는데(Table 3), 이는 A군에서 69.6%, B군에서 61.1%의 환자가 백내장 수술과 동시에 펨토초레이저를 이용한 궁상절개술을 시행받은 것과 연관이 있을 것으로 생각된다(Table 2). 펨토초레이저를 이용한 궁상절개술이 구면수차에 미치는 영향은 정립된 바가 없다. 한 연구에서는 백내장 수술과 동시에 펨토초레이저를 이용한 궁상절개술을 시행받은 환자들에서 수술 2개월 후 각막 구면수차의 값이 수술 전과 비교하여 소폭 감소 경향을 보였으나, 유의미한 차이는 없었다[20].
단초점 인공수정체를 이용한 백내장 수술 후에는 근거리 시야 확보를 위해 돋보기가 필요하지만, 상대적으로 비용이 저렴하고 원거리에서 우수한 결과를 얻을 수 있으며 후광이나 눈부심의 발생률이 낮기 때문에 여전히 널리 사용되고 있다[21,22]. 이 연구는 Primus-HD® 인공수정체가 단초점 인공수정체를 이용한 백내장 수술을 예정하고 있는 환자에게 좋은 대안이 될 수 있음을 보여준다. Primus-HD® 인공수정체는 수술 후 원거리 나안시력, 최대교정시력, 고위 수차, 술후 근시 변화부분에서 기존에 안정성이 검증된 ARTIS® PL E 인공수정체와 비슷한 결과를 보여주었고, 수술 후 구면렌즈대응치에 대한 예측력 면에서는 더 나은 예측력을 보여주었다.
본 연구의 제한점은 첫째, 제한적인 대상자 수에 대해 후향적으로 진행된 연구이기 때문에 더 많은 환자에 대한 전향적 연구가 필요할 것으로 생각된다. 둘째, 3개월간 추적 관찰을 진행하였기 때문에 더 장기간 추적관찰을 시행한 연구가 필요할 것으로 생각된다. 셋째로, 본 연구는 안축장이 22.0 mm과 26.0 mm 사이인 환자만을 대상으로 하였으므로, 안축장이 짧거나 긴 환자의 목표 디옵터 계산에 대한 추가 연구가 필요하다.
본 연구는 국내외 최초로 Primus-HD® 인공수정체의 임상 결과에 대해 보고한 연구로, Primus-HD® 인공수정체는 기존에 임상효과가 검증된 ARTIS® PL E 인공수정체와 비교하여 수술 후 1개월, 3개월의 시력 및 고위수차 측면에서 유사한 임상적 결과를 나타냈으며, 수술 후 구면렌즈대응치에 대한 예측력 면에서는 더 나은 예측력을 보여주었음을 확인하였다. 따라서 preloaded 비구면 단초점 인공수정체를 사용한 백내장 수술을 계획할 때 Primus-HD® 인공수정체가 안전하고 효과적인 후보로 사용될 수 있음을 알 수 있다.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






