
가돌림신경(abducens nerve)은 다리뇌(pons)와 숨뇌(medulla oblongata) 사이에서 거미막밑공간(subarachnoid space)으로 나와, 경사대(clivus) 위를 거의 수직으로 주행하여 해면 정맥굴로 들어가게 된다[1,2]. 경사대 위에서 가돌림신경은 팽팽하게 위치하며, 이러한 해부적 특징으로 뒤 뇌오목(posterior cranial fossa)의 외상, 수술, 종양 등의 병변에 의해서 신경마비가 발생할 수 있다[1-4]. 가돌림신경마비는 동반된 다른 눈 또는 전신 신경 증상을 확인하여, 병변의 위치와 원인을 예측할 수 있다[1,2]. 하지만, 드물게 기질적 원인에 의한 가돌림신경마비가 다른 신경 증상을 동반하지 않고 발생할 수 있다. 저자들은 다른 눈 또는 전신 신경 증상을 동반하지 않고, 작은 각의 내사시를 보인 단안 가돌림신경 마비 환자에서 경사대 척삭종을 확인하였고, 이의 수술적 치료를 통해 좋은 결과를 얻어 이를 보고하고자 한다.
증 례
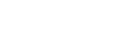
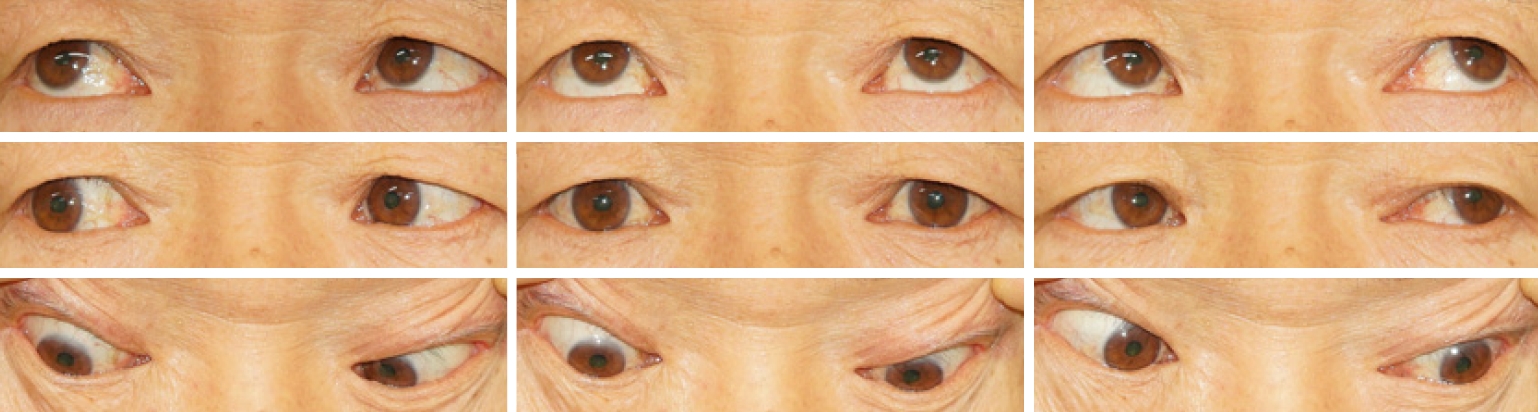
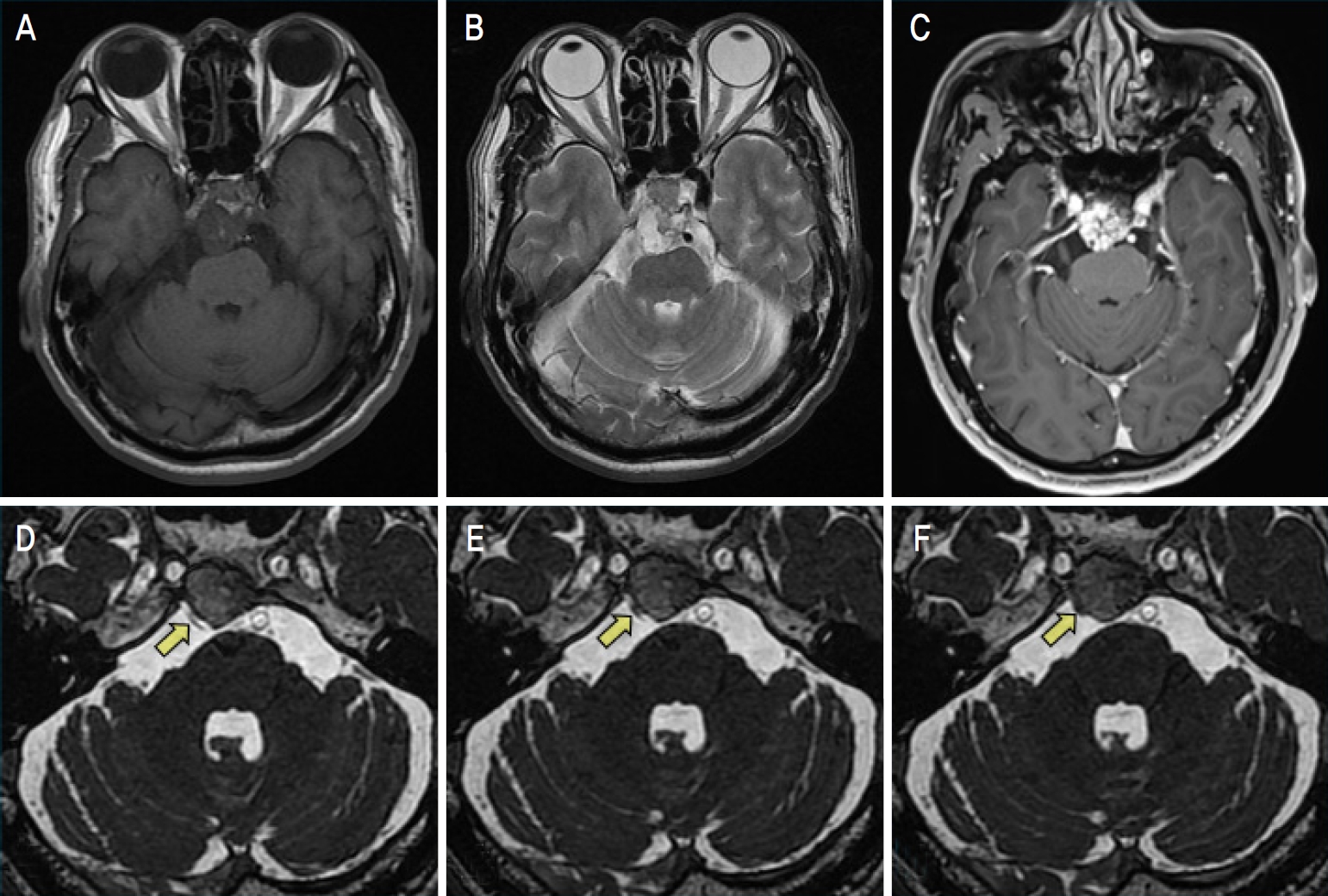
66세 남자가 4일 전 갑자기 발생한 수평두눈복시로 왔다. 증상은 일중변화(diurnal variation)를 동반하지 않았다. 이전에 복시와 사시의 안과 과거력은 없었다. 당뇨, 고혈압, 종양, 자가면역질환 등의 전신 또는 안과질환의 과거력은 없었다. 눈운동시 통증은 없었고, 관자 부위 등의 두통, 전신쇠약, 발열, 귀울림(tinnitus), 턱관절통증 및 절뚝거림(claudication) 등의 다른 전신 또는 국소 신경 증상은 없었다. 교정 시력은 양안 20/40이었다. 얼굴이상감각이나 통증은 없었다. 안검과 동공반응검사에서 이상 소견은 없었다. 안구운동검사에서 정면 주시시 6프리즘디옵터(prism diopters, PD)의 내사시를 보였다. 내사시는 우측 주시에서 12 PD로 증가하였고, 좌측 주시에서는 정위를 보였고 명확한 가쪽 운동장애는 없었다(Fig. 1). 세극등현미경검사에서 특이 소견은 없었다. 안저검사에서 특이 회선 소견이나 시신경유두부종 소견은 없었다. 복시의 원인 감별을 위해서 갑상선 호르몬수치와 항아세틸콜린수용체항체(anti-acetylcholine receptor antibody)를 포함한 혈액검사를 시행하였고, 모두 정상 범위를 보였다. 뇌자기공명영상(magnetic resonance imaging)과 자기공명혈관조영술(magnetic resonance angiography)에 우측 다리뇌 및 가돌림신경을 압박하는 경사대 종양을 확인하였다(Fig. 2). 종양의 치료를 위해 환자를 신경외과에 의뢰하였다. 종양에 대한 수술적 치료를 시행하였고, 조직검사에서 척삭종을 확인하였다(Fig. 3). 수술적 치료 후 환자는 특별한 신경학적 이상 징후가 없어 퇴원하였고 전반적 경과는 양호하였다. 수술 후 1개월째 수술 부위에 대해 방사선 치료를 시행받았으며 총 방사선량은 70 Gy를 조사받았다. 수술 후 1달 뒤 환자는 복시는 없었고, 안구운동검사에서 정위를 보였다. 수술 후 6개월에 시행한 magnetic resonance imaging (MRI)에서 종양의 재발이나 기타 이상 소견은 관찰되지 않았다.
고 찰
이 증례에서 다른 눈 또는 전신 신경 증상 없이 작은 각의 내사시를 보인 환자에서 뇌영상검사를 통해 경사대 척삭종을 진단하였고, 수술을 통해 사시와 복시의 빠른 회복을 확인하였다. 척삭종은 척삭(notochord)의 배아 잔류물에서 기원한 드문 국소 골 종양이며 주로 엉치뼈(sacrum), 목등뼈(cervical vertebra), 경사대에서 발생한다[5]. 서서히 자라지만, 국소적으로 침범하는 특성으로 낮은 또는 중등도의 악성으로 분류되며 전이는 드물다. 경사대 척사종은 경막외(extradural) 뼈에서 주로 기원하며, 눈운동과 관련하여 가돌림신경마비가 가장 많이 발생할 수 있다[5,6]. 척삭종의 위치에 따라 다양한 전신 또는 국소 신경 증상이 생길 수 있다. 하지만, 국내에서 이 증례와 같이 다른 신경 증상을 동반하지 않고 작은 각의 내사시만 보인 단안 가돌림신경 마비에서 경사대 척삭종이 진단되었던 경우는 없었다.
가돌림신경의 뇌줄기에서 눈확으로 이어지는 주행경로 중 경색(infarction), 외상(trauma), 출혈(hemorrhage), 압박(compression), 염증(inflammation) 등의 여러 원인에 의해 가돌림신경마비가 발생할 수 있다[1]. 가돌림신경은 뇌줄기 내에서는 얼굴신경(facial nerve)의 신경다발(fascicle)과 인접하고, 거미막밑공간에서는 경사대 위를 거의 수직으로 이동한다[1,2]. 해면정맥굴(cavernous sinus)을 통과할 때는 다른 뇌신경과 달리 속목동맥(internal carotid artery) 가까이 위치하고 뇌막 가쪽에 부착되어 있지 않다[7]. 이런 다양한 해부 특징으로 가돌림신경마비 환자에서 동반된 눈 또는 전신 신경 증상의 확인은 병변의 발생 부위를 예측하는 데 중요하다[1]. 이 환자에서는 뇌영상에서와 같이 우측 가돌림 신경이 거미막밑공간에서 경사대 척삭종에 의해 압박 받았고, 다리뇌는 압박 받으나 그 정도가 심하지는 않아서 다른 눈 또는 전신 신경 증상 없이 가돌림신경만 발생한 것으로 생각된다.
마비사시의 원인 감별을 위해서는 이러한 동반된 신경 증상의 확인과 함께 MRI 등의 뇌영상검사를 언제 시행할지 결정하는 것도 중요하다. 일반적으로 당뇨, 고혈압 등의 미세혈관질환의 위험 요인이 있어 허혈에 의한 마비사시로 생각되는 경우는 3개월까지 회복 여부를 확인한 후 뇌영상 검사를 시행하는 것이 제시되어 왔다[1,2]. 허혈에 의한 마비는 대개 급성으로 생기며, 3-6개월 내에 완전 회복을 보이는 경우가 많기 때문이다. 이 환자에서도 초기에 나이와 동반 증상을 고려하면 허혈에 의한 눈돌림신경마비의 가능성도 고려할 수 있었다. 환자는 고령이었고, 다른 신경 증상을 동반하지 않았으며, 내사시의 정도도 경미하였다. 그러나, 미세혈관병증의 위험 요인이 없어, 다른 원인 감별을 위해 빠른 뇌영상검사를 시행하였고, 경사대 척삭종을 확인할 수 있었다.
최근의 연구에서는 급성 마비사시와 복시 환자에서 기질 원인을 동반하는 경우는 상대적으로 적으나 허혈의 위험 요인을 통한 원인 예측에는 한계가 있을 수 있고, 적절한 치료 방향 수립을 위해서 모든 환자에서 빠른 뇌영상검사의 시행을 권유하기도 하였다[8-10]. 저자들도 기존의 임상지침 외에도 진료 환경이나 의료진의 임상 경험에 따라서 급성 마비사시와 복시 환자에서의 뇌영상검사의 시행 시기와 여부는 달라질 수 있다고 생각한다.
경사대 척삭종은 치료로 외과적 제거를 하게 되고, 근래의 내시경수술(endoscopic surgery) 기술의 발달로 이전보다 치료의 접근 범위가 넓어졌다. 완전 절제 후에도 재발의 가능성이 있어서 방사선 치료를 병행하며 지속적인 경과 관찰이 필요하다[5].
결론적으로, 전신 신경 증상 없이 작은 각의 내사시만을 보인 한눈 가돌림신경마비 환자에서 빠른 뇌영상검사를 통해 경사대 척삭종을 진단하였고, 이에 대한 수술적 치료를 통하여 좋은 결과를 확인하였다. 허혈 이외의 원인이 의심되는 경우는 가돌림신경마비의 정확한 감별진단을 위해 적극적인 뇌영상검사의 시행을 고려해야 할 것이다.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Download Citation
Download Citation Print
Print






