한 눈의 가성-신경핵사이눈근육마비로 나타난 해면정맥굴수막종 1예
Cavernous Sinus Meningioma Presenting with Unilateral Pseudo-Internuclear Ophthalmoplegia
Article information
Abstract
목적
한 눈의 가성-신경핵사이눈근육마비로 나타난 해면정맥굴수막종을 경험하였기에 이를 보고하고자 한다.
증례요약
50세 여자가 3주 전부터 서서히 시작된 정면 및 좌측 주시에서 심해지는 수평복시로 왔다. 증상은 일중 변화를 동반한다고 하며, 피곤하면 더 심해진다고 하였다. 간헐적인 우안 눈꺼풀처짐이 있었다. 원래 편두통은 있었으나 근래 더 심해졌다고 하였다. 동공 반응검사에서 정상 반응을 보였다. 안구운동검사에서 정면주시 14프리즘디옵터(prism diopters, PD)의 외사시와 우안 -1의 내전운동 장애를 보였다. 좌안의 가쪽눈떨림을 보였다. 좌측주시에서 외사시는 25 PD로 증가하였다. 임상 소견으로 가성-신경핵사이눈근육마비를 보인 눈중증근육무력증을 고려하였다. 그러나 자기공명영상을 통해 우측 해면정맥굴수막종을 확인하였고, 환자는 방사선 치료를 시행받았다. 3개월 뒤, 안구운동 소견은 정면주시에서 4 PD의 외사시로 호전되었다. 우안의 내전장애와 눈꺼풀처짐도 없었다.
결론
해면정맥굴수막종은 다양한 안구운동장애로 나타날 수 있고, 가성-신경핵사이눈근육마비도 그중 하나이다.
Trans Abstract
Purpose
We report a case of cavernous sinus meningioma presenting with unilateral pseudo-internuclear ophthalmoplegia.
Case summary
A 50-year-old female visited our clinic with a history of insidious onset of horizontal diplopia at primary and left gaze over 3 weeks. The symptom had diurnal variation and was aggravated with fatigue. There was intermittent upper eyelid drooping of the right eye. She had a history of migraines, which had recently worsened. The pupils showed a normal response to light and near stimulation in both eyes. The extraocular examination showed 14 prism diopter (PD) exotropia at primary, and 25 PD exotropia at left gaze, with -1 adduction limitation of the right eye. There was abducting nystagmus of the left eye. Ocular myasthenia gravis was suspected based on the clinical findings. Magnetic resonance imaging of the brain revealed a right cavernous sinus meningioma. The ocular symptoms improved after radiotherapy. At 3 months of follow-up, the ocular motility findings had improved to 4 PD exotropia, without adduction limitation of the right eye. The upper eyelid drooping had improved.
Conclusions
A cavernous sinus meningioma can be manifested by various types of ocular motility disorder, including pseudo-internuclear ophthalmoplegia.
신경핵사이눈근육마비(internuclear ophthalmoplegia)는 안쪽세로다발(medial longitudinal fasciculus)의 병변으로 같은 쪽 눈의 내전장애와 반대 쪽 눈의 가쪽눈떨림(abducting nystagmus)을 보인다[1,2]. 신경핵사이눈근육마비는 고령에서는 뇌경색, 젊은 성인에서는 다발경화증(multiple sclerosis) 같은 중추신경계의 국소 병변으로 발생할 수 있다[1,2].
눈중증근육무력증(ocular myasthenia gravis)은 대표적인 자가면역신경계 질환의 하나로서, 일중 변화(diurnal variation), 피로감, 눈꺼풀처짐이나 코간눈꺼풀연축(Cogan lid twitch) 등의 눈꺼풀 소견, 눈 통증을 동반하지 않는 다양한 형태의 눈운동장애를 보일 수 있다[3-5]. 눈돌림신경(oculomotor nerve) 의 지배를 받는 외안근의 신경근이음부가 눈중증근육무력 증에 영향을 받기 쉬우며, 특히 안쪽곧은근(medial rectus muscle)이 가장 흔히 침범받을 수 있다[5]. 이로 인한 가성-신경핵사이눈근육마비는 눈중증근육무력증에서 잘 발생할 수있다. 그러나 다른 다양한 원인에 의해 가성-신경핵사이눈근육마비가 발생할 수 있다[1,6-9].
해면정맥굴(cavernous sinus)을 침범하는 종양은 드물며, 이 중 수막종(meningioma)이 가장 흔하다[10]. 해면정맥굴수막종은 해면정맥굴 내의 안구운동과 관련된 뇌신경과 시신경에 영향을 주어 이와 연관된 다양한 눈증상을 발생시킬수 있다[10]. 저자들은 눈중증근육무력증에 의한 가성-신경핵사이눈근육마비로 예상한 환자에서 해면정맥굴수막종(cavernous sinus meningioma)을 진단하였기에 이를 보고하고자 한다.
증 례
50세 여자가 3주 전부터 서서히 시작된 정면 및 좌측주시에서 심해지는 수평복시로 왔다. 증상은 일중 변화를 동반한다고 하며, 피곤하면 더 심해진다고 하였다. 복시 발생후 간헐적인 우안 눈꺼풀처짐도 있다고 하였고, 안구돌출(proptosis)은 없었다. 원래 편두통은 있었으나 근래 그 정도가 더 심해졌다고 하였다. 안구통증은 없었다. 이전에 전신 질환, 종양, 감염 질환, 자가면역 질환, 외상, 약 복용, 수술 등의 과거력은 없었다. 얼굴 이상감각이나 통증은 없었다. 교정시력은 양안 20/20이었고, 색각검사에서는 정상 소견을 보였다. 동공반응검사에서 빛과 근접반사 모두 정상 반응을 보였다. 안구운동검사에서 정면 주시에서 14프리즘 디옵터(prism diopter, PD)의 외사시와 우안 -1의 내전운동 장애를 보였다(scale of -4 to 0; Fig. 1). 좌측주시에서 외사시는 25 PD로 증가하였다. 좌안의 가쪽눈떨림(abducting nystagmus)을 보였다. 눈모음(convergence)은 정상이었다. 안저검사에서 이상 소견은 없었다.
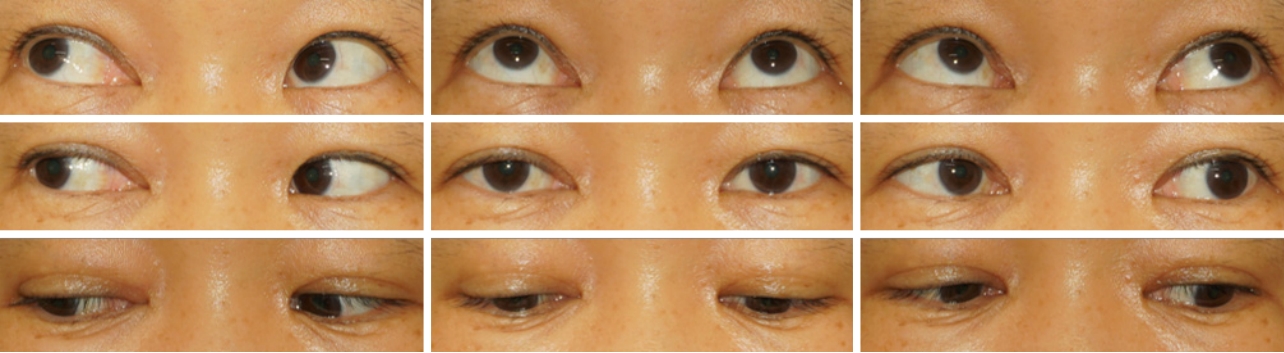
Ocular motility findings at initial visit. Image of the patient in nine diagnostic positions of gaze demonstrating 14 prism diopter (PD) exotropia at primary and 25 PD exotropia at left gaze, with -1 adduction limitation of the right eye (scale of -4 to 0). The right eye had mild ptosis.
안구운동 소견과 우안의 눈꺼풀처짐, 이러한 증상들의 일중 변화로 가성-신경핵사이눈근육마비를 보인 눈중증근육무력증 가능성을 고려하였다. 복시의 원인 감별을 위해 항아세틸콜린수용체항체를 포함한 혈액검사를 시행하였고, 정상 범위의 결과를 보였다. 뇌 자기공명영상(magnetic resonance imaging, MRI)검사를 시행하였다. 뇌 MRI에서 우측 해면정맥굴과 천막(tentorium)을 침범하는 균질(homogenous) 의 조영증강된 수막종을 확인하였다(Fig. 2). 뇌간(brainstem)의 특이 소견은 없었다. 신경외과로 의뢰되어서 방사선 치료를 시행받았고, 이후 증상은 호전되었다. 경과 관찰 3개월 뒤, 안구운동 소견은 정면주시에서 4 PD의 외사시로 호전되었고, 우안의 내전운동장애도 없었다. 눈꺼풀처짐은 없었다. 환자의 정면주시 복시에 대한 양안 2 PD 바닥안쪽프리즘(base in) 안경 처방 후 경과 관찰 중이다.
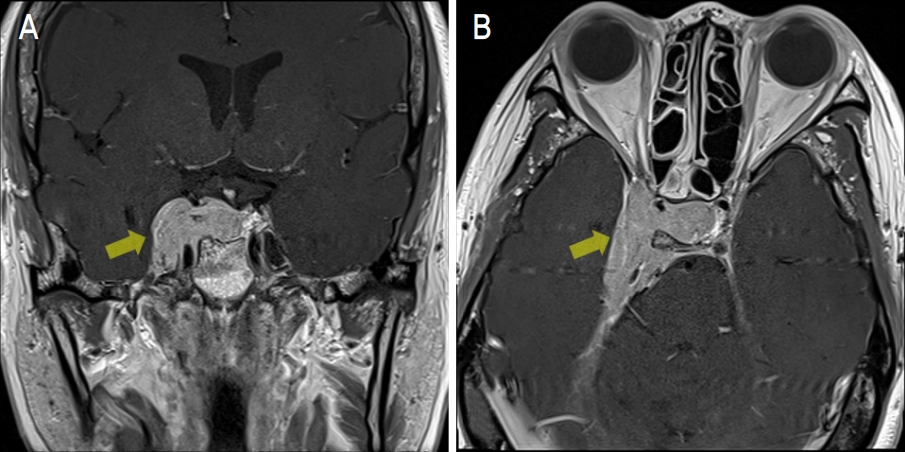
Magnetic resonance imaging of the brain demonstrated a homogenous enhancing mass (approximately 4.5 cm diameter) in the right cavernous sinus extending to the right tentorium, suggestive of a cavernous sinus meningioma. (A) Coronal view, (B) axial view (yellow arrow).
고 찰
이 증례는 일중 변화를 동반한 눈꺼풀처짐과 핵사이눈근육마비 소견을 보인 복시 환자에서 눈중증근육무력증을 의심하였으나 뇌 영상검사를 통해 해면정맥굴수막종을 진단하였던 경우다. 안쪽세로다발은 수평동향운동(conjugate horizontal eye movement)과 수직 및 회선지지(holding) 눈운동, 수직원활추종운동(vertical smooth pursuit), 수직전정눈반사(vestibuloocular reflex)에 관여한다[1]. 따라서 안쪽세로 다발의 병변은 같은 쪽 눈의 내전장애와 반대 쪽 눈의 가쪽눈떨림, 스큐편위(skew deviation)를 동반할 수 있다[1,2].0 신경핵사이눈근육마비는 정상 눈모음을 보인 내전운동 장애 소견을 확인하여 쉽게 진단할 수 있다. 하지만 안쪽곧은근에 영향을 줄 수 있는 다른 원인의 감별을 위해 내전장애뿐만 아니라 눈꺼풀 형태, 동공 반응, 내전 외 방향의 눈운동장애 동반을 확인하는 것이 중요하다.
눈중증근육무력증은 다양한 형태의 안구운동장애를 보일 수 있으며, 가성-핵사이눈근육마비는 그 중 하나로 잘 알려져 있다[3,4,11]. 눈중증근육무력증 외에도 오래된 외사시, Miller-Fischer 증후군, 안쪽곧은근의 수술적 치료 후, penicillamine 복용 후에도 가성-신경핵사이눈근육마비가 발생할 수 있다[6-9]. 그러나 이전에 가성-핵사이눈근육마비로 나타난 해면정맥굴수막종에 대한 보고는 없었다.
이 증례는 첫 진료 시 눈 소견으로 부분(partial) 눈돌림신경마비, 안와 질환, 눈중증근육무력증 등을 의심하였다. 하지만 내직근만 침범하는 눈돌림신경마비는 매우 드물며, 안구통증이나 안구돌출을 동반하지 않아서 안와 질환에 의한 가능성은 낮다고 생각하였다[12]. 환자의 안구운동 소견과 복시의 일중 변화, 눈꺼풀처짐이 있어서 눈중증근육무력증의 가능성이 높다고 생각하였다. 그러나 뇌 영상검사를 통해 해면정맥굴수막종을 진단할 수 있었다.
수막종은 해면정맥굴에서 발생하는 가장 흔한 종양이다[10]. 해면정맥굴은 다양한 크기의 정맥이 분할과 융합된 얼기(plexus) 공간 내에 속목동맥, 눈돌림신경, 도르래신경(trochlear nerve), 가돌림신경(abducens nerve), 교감신경(sympathetic carotid plexus), 삼차신경(trigeminal nerve)이 밀집해 있는 해부적 특징을 가지고 있다. 이에 해면정맥굴수막종은 시신경이나 안구운동 관련 신경에 영향을 주어, 시력저하, 안구운동마비에 의한 복시, 두통, 뇌하수체기능 부족(pituitary insufficiency) 등의 증상이 발생할 수 있다. 해면정맥굴수막종이 주위 신경혈관조직을 직접 침범 또는 압박을 통해 증상을 유발하며, 안구운동장애는 가돌림신경 마비와 눈돌림신경마비가 주로 발생할 수 있다[10]. 이 환자의 경우도 수막종이 눈돌림신경에 부분적으로 영향을 주어 눈꺼풀처짐과 안구운동장애가 발생하였을 것이다. 대부분 병변의 직접적인 조직검사보다는 영상검사의 결과로 진단할 수 있다[10]. 해면정맥굴수막종은 대부분 안정적이나 초기의 병변 크기와 그 증가가 신경 증상 발생과 일치하는 것은 아니다. 신경 증상 발생에 따라 치료 여부를 결정하게 되고, 혈관이나 신경 구조물 손상에 의한 합병증 발생 가능성으로 직접적인 수술보다는 방사선 치료가 주로 이루어진다[13]. 초기에 신경 증상에 대해서 단기간 스테로이드 치료를 고려할 수도 있다[10].
눈중증근육무력증는 임상적 진단이며, 혈청검사 외에도 얼음검사(ice test), 휴식검사(rest test), 전기생리검사(electrophysiology test) 등이 진단에 도움을 줄 수 있다[3,4]. 환자가 호소한 증상의 일중 변화가 중증근무력증의 가능성을 시사하는 소견이었지만, 얼음검사나 휴식검사 또는 시간에 따른 사시각 변화의 측정 등을 시행하지 않아 일중 변화가 있다는 객관적 증거는 확인하지 못하였고, 본 증례에서 증상의 일중 변화의 원인은 알 수 없었다. 눈중증근육무력증이 의심되는 환자에서 뇌 영상검사는 여러 진단 검사들 중 첫 고려 대상은 아닐 것이다. 또한, 해면정맥굴수막종에서도 초기의 스테로이드 치료로 안구운동장애와 복시 증상이 호전될 수 있다[10]. 눈중증근육무력증은 다양한 안구운동장애 소견으로 나타날 수 있고, 특발안와염(idiopathic orbital inflammation) 등의 다른 자가면역 질환과 동반되어 발생할 수 있다[3,14]. 따라서, 안구통증, 안구돌출(proptosis) 등의 다른 눈 증상이나 두통, 귀울림(tinnitus) 등의 비전형적인 신경 증상이 동반된다면, 다른 원인 질환을 감별하기 위해 안와를 포함한 뇌영상검사를 적극적으로 시행하는 것이 필요할 것이다[15]. 결론적으로 해면정맥굴수막종에서 가성-신경핵사이눈근육마비가 발생할 수 있음을 확인하였다.
Notes
The authors have no conflicts to disclose.