쇼그렌 및 비쇼그렌증후군 환자에서 안구표면염색점수와 혈중 비타민 D 농도의 상관관계 비교
Correlation between Ocular Surface Staining Score and Serum Vitamin D in Sjögren’s and Non-Sjögren’s Syndrome
Article information
Trans Abstract
Purpose
To analyze the correlation between the ocular surface staining score (OSS) and serum vitamin D level for patients of Sjögren's syndrome (group A) and non-Sjögren's syndrome (group B) with dry eye symptoms.
Methods
In this observational cross-sectional study, The Schirmer I test, OSS, tear film break-up time and serum vitamin D level were measured in 65 eyes of 65 adults complaining of dry eye. Among 65 people, 35 people in group A and 30 people in group B. The Student’s t-test was used for analyzing the ocular surface staining respectively, in group A and group B patients. Pearson’s correlation was used to analyze the correlations of OSS with serum vitamin D level.
Results
The serum vitamin D level (rho = -0.245, p = 0.049) was negatively correlated with OSSs. Especially, the serum vitamin D level (rho = -0.440, p = 0.008) was significantly negatively correlated with OSSs in Sjögren's syndrome patients even more than total patient group.
Conclusions
This suggests that the OSS is highly related to immunological factors such as vitamin D in dry eyes due to an underlying immunological disease. Finding the exact relationship between the inducer of dry eye and the degree of dry eye and clarifying the correlation seems to play an important role in the direction of treatment for dry eye.
쇼그렌증후군(Sjögren’s syndrome)은 외분비샘의 기능에 영향을 미치는 자가면역질환의 하나로써, 건성안으로 인한 각결막염 및 구강 건조증을 초래한다. 특히, 눈물샘에 림프구 침윤이 발생하고, 눈물의 분비 기능이 감소하게 된다. 쇼그렌증후군은 다른 류마티스질환 없이 원발성으로 발현되는 일차 쇼그렌증후군과 류마티스 관절염, 전신 홍반루푸스 등 다른 자가면역질환으로 유발되는 이차 쇼그렌증후군이 있다[1]. 쇼그렌증후군의 진단 기준 중 2016 American College of Rheumatology-European League Against Rheumatism (ACR-EULAR) criteria (Table 1)을 살펴보면, 안구표면염색점수(ocular surface staining score, OSS)와 쉬르머검사(Schirmer I test)가 진단 기준에 포함됨을 확인할 수 있고, 건성안은 쇼그렌증후군 진단에 있어 중요한 부분을 차지하고 있다.

2016 American College of Rheumatology-European League Against Rheumatism criteria
안과학적으로 안구건조증과 혈중 비타민 D의 관계에 대해 여러 연구를 해 온 바 있다[2]. 비타민 D는 면역 반응을 조절하는 경향이 있으며, 혈중 비타민 D 농도가 낮을수록 자가면역질환, 림프종, 신경병증 등과 관련 있음이 증명되었다. 특히, Lee et al [3]은 쇼그렌증후군이 동반된 건성안 환자에서 일반적인 건성안 환자에 비하여 혈중 비타민 D 농도가 유의하게 낮음을 보고한 바 있다. 또한, Kurtul et al [4]은 쇼그렌증후군이 아닌 건성안 환자군에서 혈중 내 비타민 D 농도가 감소한 경우 쉬르머검사와 눈물막파괴시간이 단축된 것을 보고한 바 있다. 그러나 국내의 앞선 연구들에서 눈마름 임상증상을 보이는 쇼그렌증후군 및 비쇼그렌증후군(non-Sjögren’s syndrome) 환자에서 안구표면염색점수와 혈중 비타민 D 농도 간의 상관관계 및 비교에 대해서는 발표된 바 없어 본 연구에서 분석하고자 한다.
대상과 방법
본 연구는 단면 연구(cross-sectional study)로써 2017년 7월부터 2019년 4월까지 류마티스 내과에서 쇼그렌증후군으로의 진단을 위해 의뢰된 환자 중 건성안 증상(건조감, 따가움, 이물감)과 입마름 증상(빈번한 갈증, 입과 목의 건조감, 입과 혀의 작열감 혹은 저린 느낌, 입술 갈라짐)을 호소하는 환자들을 대상으로 하였다. ACR-EULAR criteria에 따라 이들 중 쇼그렌증후군으로 진단받은 환자(A군)는 35명이고, 건성안 증상과 입마름 증상을 호소하지만 쇼그렌증후군이 아니라고 진단받은 환자(B군)는 30명이었다.
이전에 진단받은 안과적 질환이 있거나 2등급 이상의 마이봄샘 기능부전(meibomian gland dysfunction), 6개월 이내에 알레르기결막염(allergic conjunctivitis) 혹은 안과 수술을 받은 경우, 3개월 이내에 콘택트렌즈를 착용한 경우, 누점마개(punctal plug)를 삽입한 경우, 인공눈물 외에 다른 안약을 점안하는 치료를 받은 경우, 당뇨, 고혈압, 갑상선질환, 알레르기질환, 우울장애 등 전신질환으로 약을 복용하는 경우 대상에서 제외하였다. 본 연구는 헬싱키선언에 입각한 인천성모병원의 의학연구윤리심의위원회(Institutional Review Board, IRB)로부터 승인번호 OC20RASI0041로 심의 승인을 받아 연구를 시행하였다.
쇼그렌증후군을 진단하는 기준은 가장 최근에 개정된 2016 ACR-EULAR criteria (Table 1)을 사용하였으며, 안구표면염색점수는 형광물질(Fluorescein®; Haag-Streit International, Koniz, Switzerland) 염색약으로 각막과 결막을 염색하여 Sjögren's International Collaborative Clinical Alliance Ocular Staining Score (Fig. 1)에 따라 각막과 결막에 염색되는 점상의 미란 정도에 따라 각막, 결막에 대해 각각 0-6점, 총 0-12점으로 점수화하였다. 안구표면염색점수는 같은 검사자에 의해 이루어졌다.
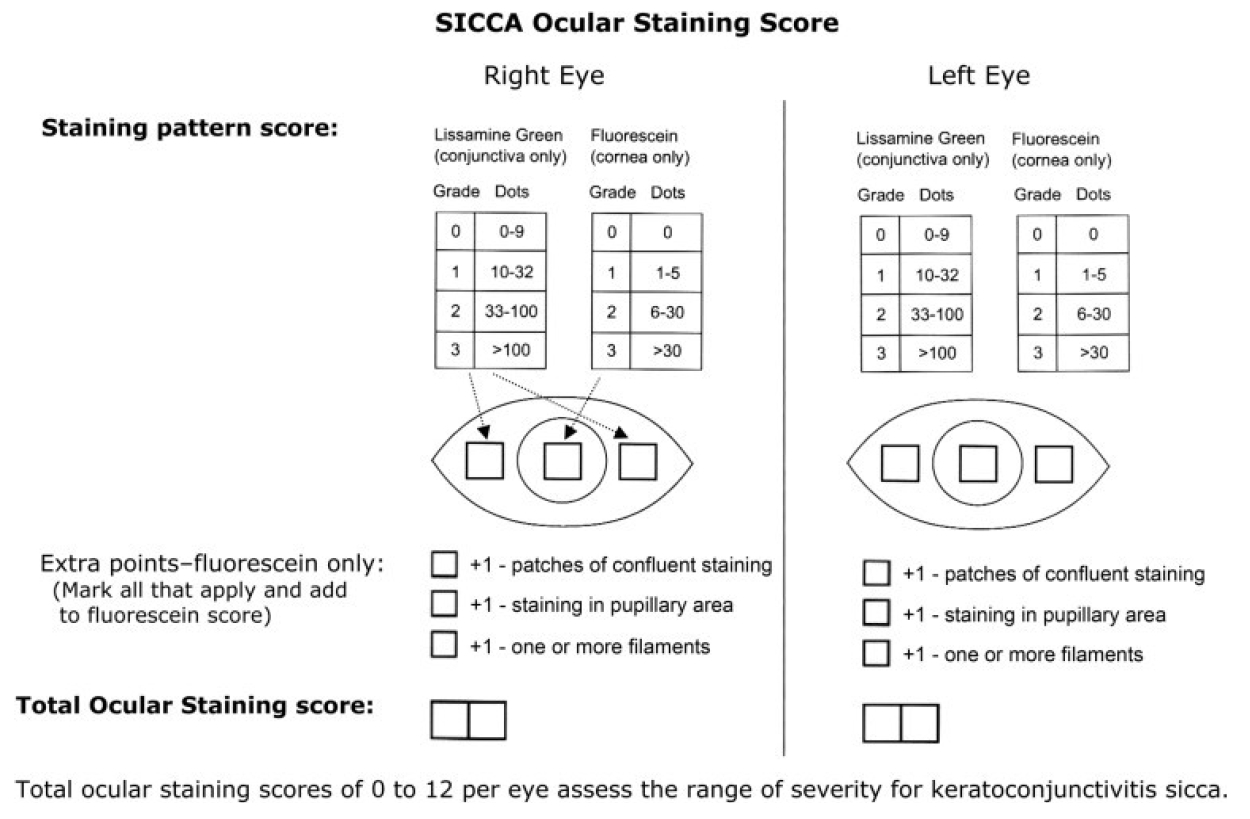
Sjögren's International Collaborative Clinical Alliance (SICCA) ocular staining score form. Ocular surface staining is assessed using fluorescein dye for the cornea and lissamine green dye for the conjunctiva.
혈중 비타민 D 농도는 혈중 25(OH)D3 농도를 화학발광면역분석 기술(chemiluminescent immunoassay technology; Siemens AG, Erlangen, Germany)로 측정하였다. 혈중 25 (OH) D3 농도는 통상 30 ng/mL 초과를 정상 수치로 간주한다.
쉬르머검사는 점안마취를 이용하지 않았으며, 검사지를 아래 결막구석 바깥 1/3 지점에 둔 후, 5분이 지나고 검사지를 제거한 후 젖은 부분의 최대 지점의 길이를 mm로 측정하였다. 검사지는 Schirmer tear® (EagleVision Inc., Menphis, TN, USA)를 이용하였다.
통계는 SPSS 통계프로그램(version 18.0; IBM Corp., Armonk, NY, USA)을 사용하였으며, A군과 B군 간에 안구표면염색점수와 혈액 중 비타민 D 농도의 차이가 있는지에 대한 비교에는 Student t-test를 사용하였고, 안구표면염색점수와 혈액 중 비타민 D 농도 지표 간의 상관분석 및 쉬르머검사와 혈액 중 비타민 D 농도 지표 간의 상관분석은 Pearson’s correlation을 사용하였으며, 모든 통계 분석은 p-value가 0.05 미만일 경우를 통계적으로 유의한 것으로 간주하였다.
결 과
본 연구는 총 65명, 65안을 대상으로 진행되었으며, 전체 대상자 중 남성 3명(4.62%), 여성 62명(95.38%)으로 눈마름 임상증상을 호소하는 환자 중 여성이 절대적으로 높은 비율을 차지하였으며, 평균 연령은 54.23 ± 13.45세였다. 혈중 비타민 D 농도의 평균은 21.22 ± 8.34 ng/mL, 안구표면염색점수의 평균은 3.32 ± 2.09, 쉬르머검사의 평균은 4.23 ± 2.28 mm였으며, 전체 대상자의 연령, 성별, 혈중 비타민 D 농도, 안구표면염색점수, 쉬르머검사 등 각 지표의 평균 분포는 Table 2에 정리되어 있다.
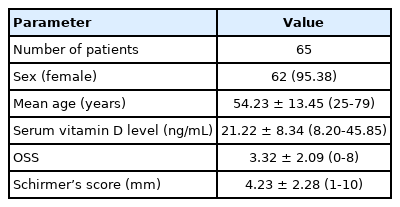
Clinical characteristics of study population
안구표면염색점수(p<0.001)의 평균은 A군은 4.29 ± 2.11, B군은 2.2 ± 1.42로 두 군 간에 통계적으로 유의한 차이가 있었으나 혈중 비타민 D 농도(p=0.301)의 평균은 A군은 20.63 ± 9.08 ng/mL, B군은 21.90 ± 7.48 ng/mL로 통계적으로 유의한 차이가 없었다. 쉬르머검사 수치(p=0.004)의 평균은 A군은 3.49 ± 2.20 mm였으며, B군은 5.10 ± 2.09 mm였다(Table 3). 혈액 중 비타민 D 농도(p=0.663)는 안구표면염색점수를 제어 변수로 하였을 때도 두 군 간에 통계적으로 유의한 차이가 없었다.

Comparison of clinical measurements between different disease groups
쉬르머검사 수치와 혈액 중 비타민 D 농도 지표 간의 상관관계를 분석한 결과, 혈액 중 비타민 D 농도(rho=0.396, p=0.001)는 쉬르머검사 수치과 통계적으로 유의한 양의 상관관계를 보였다. A군과 B군 각각에서 비교한 결과, 혈액 중 비타민 D 농도와 쉬르머검사 수치와의 관계는 A군(rho=0.391, p=0.020)과 B군(rho=0.407, p=0.026)에서 모두 통계적으로 유의한 양의 상관관계를 보였다.
안구표면염색점수와 혈액 중 비타민 D 농도 지표 간의 상관관계를 분석한 결과, 혈액 중 비타민 D 농도(rho=-0.245, p=0.049)는 안구표면염색점수와 통계적으로 유의한 음의 상관관계를 보였다(Fig. 2). A군과 B군 각각에서 비교한 결과, A군에서는 혈액 중 비타민 D 농도(rho=-0.440, p=0.008)는 안구표면염색점수와 통계적으로 유의한 음의 상관관계를 보였으며, 나이를 제어 변수로 하였을 때도 음의 상관관계(rho=-0.347, p=0.044)를 나타냈다. A군에서는 전체를 대상으로 하였을 때보다 음의 상관관계가 더 강하게 나타남을 확인할 수 있었다. B군에서는 통계적으로 유의하지 않은 양의 상관관계(rho=0.179, p=0.343)를 보였으며, 나이를 제어 변수로 하였을 때도 통계적으로 유의하지 않은 양의 상관관계(rho=0.191, p=0.320)를 보였다.

Association between ocular surface staining score (OSS) and serum vitamin D level. In all subjects, OSS was negatively correlated with serum vitamin D level. (A) In all subjects, OSS was negatively correlated with serum vitamin D level. (B) In Sjögren disease group, OSS was significantly negatively correlated with serum vitamin D level. (C) In non-sjögren disease group, OSS was not correlated serum vitamin D level. Data were analyzed using Pearson’s correlation.
고 찰
쇼그렌증후군은 면역세포의 활성화와 자가면역 활동 및 유전학적 기반을 발생 기전으로 하는 전신에 진행되는 자가면역질환이다. 면역 반응이 외분비샘에 과도하게 발생하여 전형적인 건조증이 발생하게 된다. 다른 쇼그렌증후군의 임상양상으로는 피로, 근골격계 증상, 피부 증상, 폐의 침윤, 소화기계 증상, 신증후군, 신경학적 증상, 혈액학적, 종약학적 증상 등 다양하게 나타난다[5]. 현재 쇼그렌증후군의 치료로 대증적 치료부터 전신 면역억제 치료까지 다양하게 있으며, 최근 비타민 D 보충제가 쇼그렌증후군 치료에 효과적임이 알려진 바 있다[2]. 또한 비타민 D는 면역조절 효과가 있으며, 자가면역질환에서 비타민 D 결핍 유병률이 높음은 여러 연구를 통해 알려진 바 있다[6]. 그리고 Yildirim et al [7]은 비타민 D 결핍 환자에서 건성안 인자에 대해 조사한 결과 혈중 비타민 D 농도와 건성안 인자가 유의하게 음의 상관관계를 나타냄을 보고한 바 있다. 기존 연구에서는 자가면역질환을 가진 환자군에서 비타민 D 농도가 유의하게 낮음이 보고되어 있으나, 본 연구에서는 쇼그렌증후군과 쇼그렌증후군이 아니라고 진단받은 환자에서 비타민 D의 농도가 유의하게 다르지 않아 비타민 D 농도와 안구표면염색점수의 상관관계의 비교에 각 군의 비타민 D 농도가 영향을 주지 않았다. 그럼에도 불구하고 쇼그렌증후군에서 비타민 D 농도와 안구표면염색점수가 더욱 음의 상관관계를 가짐을 확인할 수 있었다.
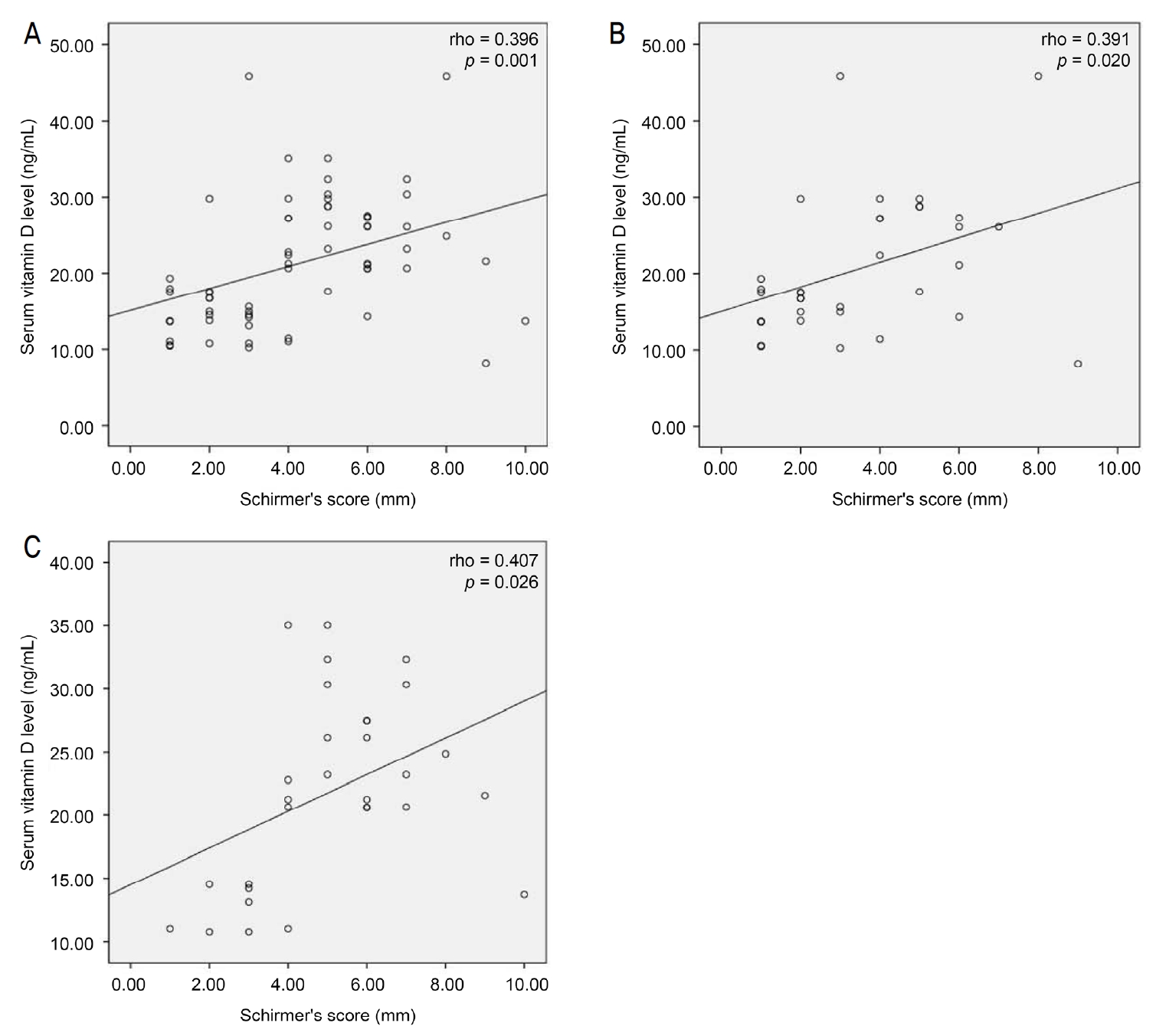
Association between Schirmer’s score and serum vitamin D level. In all subjects, ocular surface staining score was positively correlated with serum vitamin D level (A). Schirmer’s score was positively correlated with serum vitamin D level in Sjögren disease group (B) and non-Sjögren disease group (C). Data were analyzed using Pearson’s correlation.
비타민 D3는 피부에서 자외선을 통해 합성되며, 식이로도 섭취할 수 있다. 이런 비타민 D는 여러 형태로 체내에 존재하며, 이 중 혈중 25(OH)D3의 농도가 체내 비타민 D 양을 나타내는 가장 신뢰할 만한 수치이다[8]. 비타민 D의 면역조절 효과는 T 림프구를 조절함으로써 발생하는 것으로 알려져 있으며, 따라서 비타민 D의 부족은 T 림프구 및 T 림프구가 조절하는 면역 세포들의 침윤으로 나타나게 된다[6].
건성안은 눈물의 높은 삼투압, 염증 반응 및 기계적으로도 눈물막, 각막상피, 상피하 신경총에 악영향을 준다. Dry Eye Workshop의 보고서에 따르면 눈물의 삼투압은 건성안에서 가장 중요한 객관적 지표 중 하나이며, 안구표면손상의 기전에서 중추적인 기전으로 간주되어야 한다. 눈물의 고삼투압은 상피세포의 사멸을 자극하고, 염증 반응을 유발하며, 점액(mucin)을 분비하는 술잔세포(goblet cell)의 손실을 야기한다. 이는 눈물막(tear film)의 불안정성을 악화시키며 안구표면에 손상을 주는 악순환을 야기한다[2]. 비타민 D는 사람의 cathelicidin (LL-37) 등을 포함한 항미생물 펩타이드(antimicrobial peptide)를 유발하여 세포 면역 체계를 증강시킨다. 특히 cathelicidine는 각막 및 결막의 표피세표에서 분비되며, 각결막의 표면에서 면역 인자 중 가장 효과적인 감염원에 대한 장벽으로 연구된 바 있다[9].
눈마름을 호소하는 환자들에서 비타민 D 보충제의 복용에 대한 연구가 여럿 진행되었다. Bae et al [9]은 비타민 D 보충제를 복용하기 이전에 비하여, 비타민 D를 복용한 2-6주 후에 눈물막파괴시간, 안구표면염색점수, 쉬르머검사의 수치는 증가하였고, 눈꺼풀 테두리의 충혈 및 안구표면질환지수(Ocular Surface Disease Index)는 감소하였음을 보고한 바 있다. 더불어 일일 800 IU 이상의 비타민 D의 경구 복용이 6-12개월 이후 비타민 D 결핍군 및 고령에서도 혈중 25(OH)D3 농도의 기준치를 높여주는 것이 보고된 바 있으며[10], 비타민 D 결핍이 있는 류마티스질환 환자들에서 300,000 IU의 고농도 경구 비타민 D 복용이 3-6개월 후 혈중 25(OH)D3 농도의 기준치를 높인 것이 보고된 바 있다[11].
건성안을 유발하는 인자들은 다양하며, 특히 면역과 관련된 건성안에서는 다른 건성안에서 보다 안구표면염색점수가 유의미하게 높으며, 눈물막파괴시간, 쉬르머검사가 유의미하게 낮고, 각막 신경섬유세포가 적으며, 국소적 림프구가 증가했음이 보고된 바 있다[12]. 따라서 건성안의 유발인자와 건성안의 정도에 관한 정확한 관계의 파악 및 상관관계의 규명은 건성안 치료의 방향에 중요한 역할을 할 것으로 보인다.
쇼그렌증후군과 혈중 비타민 D 농도와의 관련성에 대해서는 논란이 있었다. Baldini et al [13]은 쇼그렌증후군 환자에서 혈중 비타민 D 농도가 비쇼그렌증후군에 비교하여 차이가 없다고 보고한 바 있다. 하지만 Bang et al [14]은 비쇼그렌증후군과 비교하여, 쇼그렌증후군 환자들의 혈중 비타민 D 농도가 더 낮으며, 심지어 쇼그렌증후군의 활성 정도와 비타민 D 결핍이 관련되어 있음을 보고하였다. Kuo et al [15]은 일차 쇼그렌증후군 환자에서 메타 연구를 시행하였으며, 비타민 D 결핍인 환자에서 눈물막파괴시간이 짧아지고, 쉬르머검사 수치가 더 작아지며, 안구표면염색점수는 더 높아짐을 보고하였다. 이렇듯 아직 쇼그렌증후군에서 혈중 비타민 D 농도는 논란이 있으며, 본 연구에서는 눈마름을 호소하는 환자군에서 건성안의 객관적 지표인 안구표면염색점수가 비타민 D와 음의 상관관계를 가지며, 특히 쇼그렌증후군에서는 그 음의 상관관계가 더 강하게 나타남을 보고하는 바이다.
본 연구에서는 환자들의 영양 상태에 따른 정보가 통제되지 않은 점에서 한계를 가진다. 앞서 언급하였듯 혈중 비타민 D의 농도는 비타민 D의 경구 복용량에 영향을 받는다. 또한 비타민 D는 경구 복용 외에도 피부에서 합성되는 등의 여러 획득 경로가 있어 환자의 영양 및 생활에 대해서도 통제된 연구가 필요할 것으로 사료된다. 또한, 본 연구에서 건성안의 정도를 객관적으로 수치화한 검사법으로 안구표면염색점수를 사용하였는데, 이외에도 눈물 내 싸이토카인 농도, 결막 술잔세포의 압흔세포법(impression cytology) 등 건성안과 관련된 다른 면역학적 지표들[16]에 대해서도 상관관계에 대한 추가 연구가 필요할 것으로 사료된다.
Notes
The authors have no conflicts to disclose.