비전형적 양상을 보이는 눈개회충증에 의한 단안 시신경병증
Atypical Form of Unilateral Optic Neuropathy Caused by Ocular Toxocariasis
Article information
Abstract
목적
눈개회충증으로 인한 비전형적 양상을 보이는 단안 시신경병증을 경험하였기에 증례를 보고하고자 한다.
증례요약
75세 남환이 최근 발생한 우안 시력저하를 주소로 내원하였다. 우안 시력 0.4로 측정되었으며 상대적동공산대반응 양성 소견 관찰되었다. 세극등현미경검사에서 전방 내 염증 소견 및 유리체세포 및 유리체 흐림 소견이 관찰되었다. 안저검사에서 우안 시신경 부종 및 시신경 주위 국소망막염 소견이 관찰되었다. 형광안저혈관조영술에서 시신경유두 부근 누출 소견과 함께 국소망막염 소견을 보였다. 혈청학적 검사에서 toxocara IgG가 양성이었다. 비전형적 양상의 눈개회충증 의심 하에 국소 및 경구 스테로이드, 알벤다졸 치료 후 경과 관찰하였다. 이후 시신경 부종 및 유리체염증은 호전을 보였으나, 시신경유두가 창백해지고 중심시야 결손을 동반하여 최종 시력은 0.125로 측정되었다.
결론
시신경염이 의심되는 환자에서 전방, 유리체의 염증과 포도막염이 동반되어 나타나는 경우 눈개회충증이 비전형적인 형태로 발현될 수 있으며 비가역적인 시신경 손상으로 나쁜 예후를 보일 수 있는 바 주의를 요한다.
Trans Abstract
Purpose
To report an atypical form of ocular toxocariasis presenting as unilateral optic neuropathy.
Case summary
A 75-year-old man was referred to our clinic owing to the recently developed visual difficulty in his right eye. The visual acuity of the right eye was 0.4, a relative afferent pupillary defect was positive in the right eye. On slit lamp biomicroscopy, anterior chamber inflammation and vitreous cells and haze were detected in the right eye. On fundus examination, optic disc swelling and focal retinitis around the optic disc were found in the right eye. Fluorescein angiography revealed focal retinitis along with leakage near the optic disc in the right eye. Serology was positive for Toxocara IgG. Under the suspicion of an atypical form of ocular toxocariasis, the patient was treated with local and oral steroids and albendazole. Subsequently, optic disc swelling and vitreous inflammation improved, but the final visual acuity was 0.125 with pale optic disc and central visual field defects in the right eye.
Conclusion
In patients suspected of optic neuritis, when the anterior chamber and vitreous inflammation and uveitis are accompanied, ocular toxocariasis can present atypically and requires attention because may have a bad prognosis owing to irreversible optic nerve damage.
눈개회충증은 고양이나 개의 회충인 Toxocara canis의 유충의 우연한 섭취로 인해 발생하는 안구 기생충 질환이다[1]. 눈개회충증은 전형적인 안과적 임상 양상, 혈청학적 검사 결과, 그리고 이외 안구 육아종성 질환을 배제함으로써 임상적으로 진단된다[2]. 눈개회충증의 전형적인 안과적 임상양상은 주로 단안을 침범하며, 후극부 또는 주변부 망막의 육아종성 병변이 관찰되며, 망막전막, 황반부종, 망막박리, 유리체망막 견인, 유리체혼탁 등 다양한 임상 양상을 동반할 수 있으며 비전형적 안과적인 임상양상으로는 시신경 육아종, 시신경염 또는 망막 밑으로 움직이는 개회충 소견으로 나타날 수 있다[2,3].
본 증례에서는 비전형적 양상을 보이는 눈개회충증에 의한 단안 시신경병증을 진단하고 치료 했음에도 불구하고 비가역적인 시신경 위축으로 진행하는 증례를 경험하였기에 이를 보고하고자 한다.
증 례
75세 남환이 최근 발생한 우안 시력저하를 주소로 응급실을 경유하여 안과 진료를 시행하였다. 안과 수술, 안외상을 포함한 안과적 과거력 및 전신질환 과거력은 없었다. 응급실 진료에서 우안의 시신경염이 의심되어 촬영한 뇌-안와 자기공명영상촬영(magnetic resonance imaging)은 정상이었다. 초진 시 시행한 안과검사에서 교정시력 우안 0.4, 좌안 0.63이었고 안압은 우안 18 mmHg, 좌안 21 mmHg였다. 안구운동검사에서 정상 소견을 보였으며 안구 움직임에 통증을 호소하지 않았다. 대광반사는 관찰되었으나 우안 상대구심동공운동장애에서는 양성소견으로 관찰되었다. 양안에 각각 시행한 이시하라 색각검사(Ishihara’s test for color deficiency, 24 plates edition, 2005; Kanehara & Co, Ltd, Tokyo, Japan)에서 모두 정상이었으나 우안에 경도의 색감 저하를 호소하였다. 세극등현미경검사에서 우안 전방내 염증 및 유리체세포는 1+ 관찰되었고 유리체 흐림 소견이 관찰되었다. 안저검사에서 우안 비대칭적 양상의 시신경유두 부종 및 시신경 주위 국소망막염 소견, 형광안저혈관조영술에서 시신경유두 부근 이측부에 부채꼴 모양의 누출 소견과 함께 국소망막염 소견을 보였으며, 시신경유두 부근 누출은 이측부가 심한 비대칭적 소견을 보였다(Fig. 1). 빛간섭단층촬영에서 우안 시신경유두 부근의 망막신경섬유층과 신경절세포-내망상층의 두께 증가가 관찰되었다. 시야검사(Humphrey Field Analyzer; Carl Zeiss Medictec Inc., Dublin, OH, USA)에서 우안 상측 활모양 암점, 비측 암점이 관찰되었다(Fig. 2). 우안의 포도막염 및 시신경유두 부종의 원인을 감별하기 위해 면역혈청검사를 포함한 혈액검사를 시행하였다.
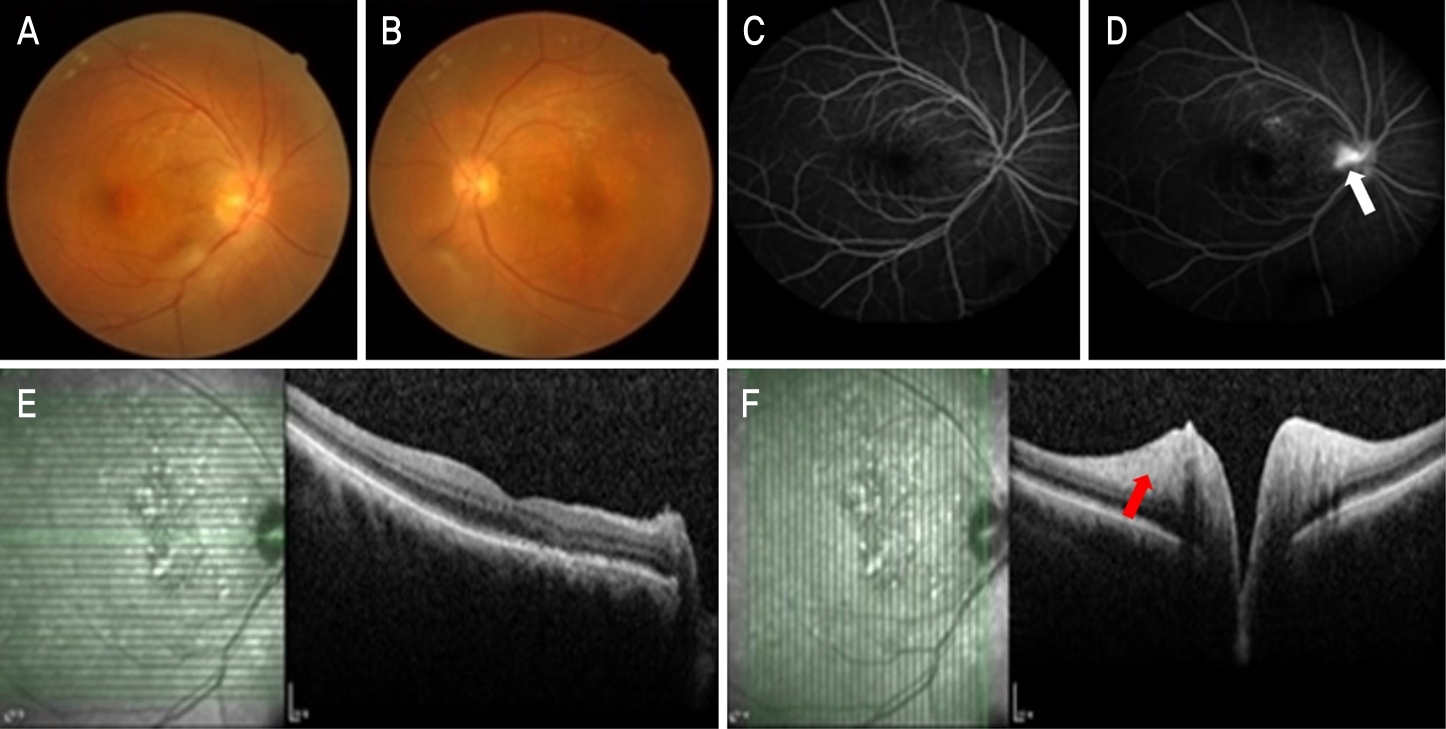
Fundus photography, fluorescein angiography (FAG), and optical coherence tomography (OCT) at initial presentation. Fundus photography shows asymmetric optic disc edema in right eye (A, B). FAG reveals sectorial late disc leakage (white arrow) in right eye (C, D). OCT shows increased thickness of the retinal nerve fiber layer and ganglion cell-inner plexiform layer (red arrow) in right eye (E, F).
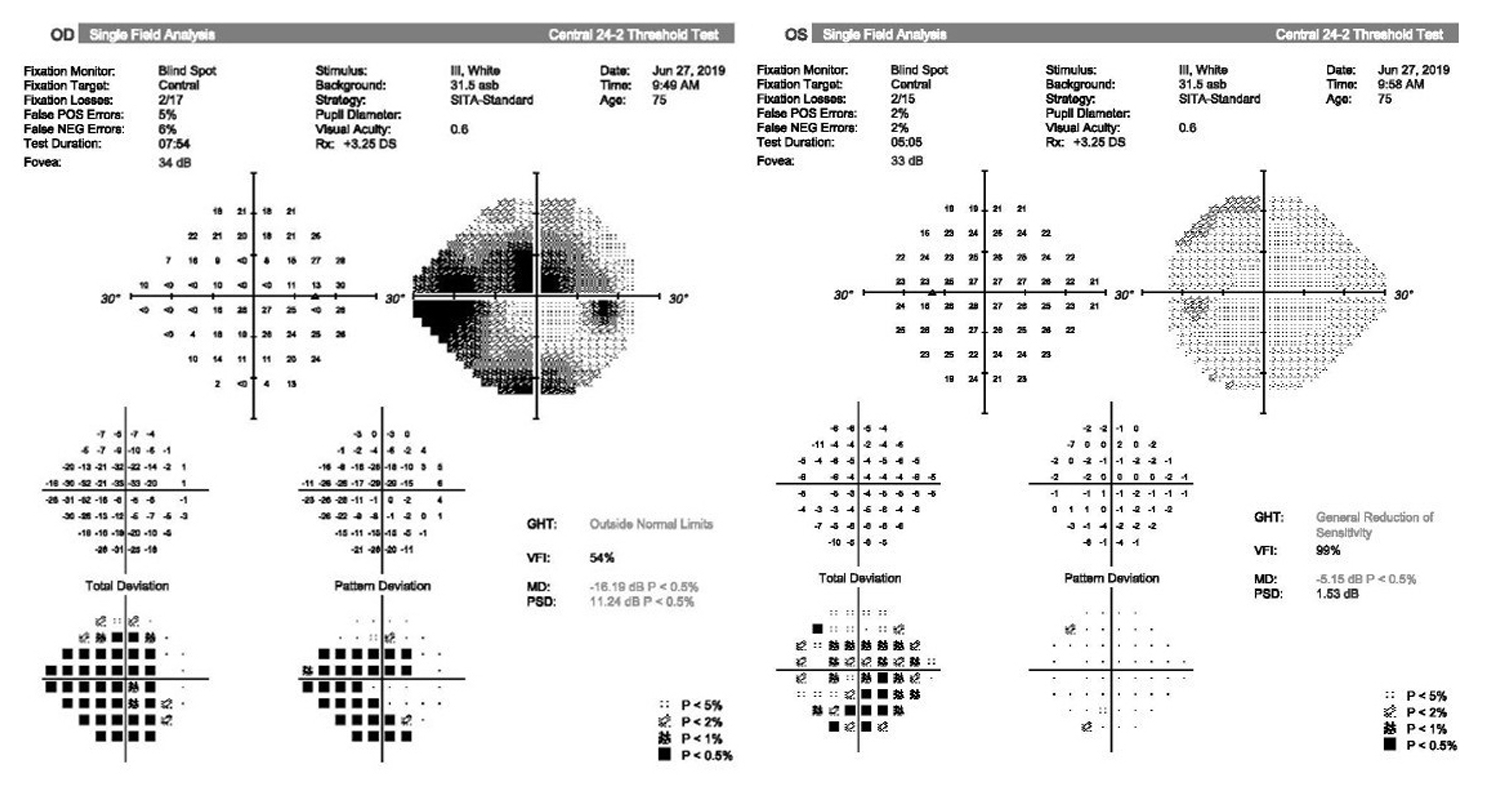
Visual field examination at initial presentation demonstrates superior arcuate defect and nasal defect in right eye.
1주일 후 내원 시 교정시력은 우안 0.1, 좌안 0.5였고 안압은 우안 19 mmHg, 좌안 16 mmHg였다. 안저검사에서 우안의 이측으로 새로운 시신경유두출혈 및 시신경유두창백이 관찰되었다. 혈청학적 검사 결과에서 syphilis, toxoplasma, IGRA는 모두 음성이었으며 toxocara IgG가 양성이었다. 추가적인 문진 결과 환자는 마당에 커다란 개를 키우고 있었으며, 평소 생간을 복용하는 식이습관이 있는 것을 확인하였다. 이에 병력 및 검사 소견을 종합하여 우안의 toxocara optic neuropathy로 진단하였다. 알벤다졸(albendazole) 400 mg 2회/일을 14일에 걸쳐 경구 투여하였으며, 프레드니솔론(prednisolone) 60 mg 1회/일을 경구 투여 시작하였다. 전방내 염증이 관찰되어 0.5% levofloxacin (Cravit®; Santen Pharmaceutical Co., Ltd, Osaka, Japan) 4회/일과 1% prednisolone (Pred-forte®; Allergan Korea Ltd., Seoul, Korea) 4회/일을 우안에 점안 시작하였다.
치료 시작 4주 후 우안 시력은 0.1로 동일하였으나 안저검사에서 우안의 유두함몰이 관찰되며 시신경유두부종의 호전을 보였으며 빛간섭단층촬영에서 우안 망막신경섬유층과 신경절세포-내망상층의 두께 감소를 보였다(Fig. 3). 경구 프레드니솔론 60 mg 1회/일을 2주 단위로 10 mg/일씩 감량하였다. 그리고 안저검사에서 우안의 시신경유두출혈 및 유두함몰이 관찰되었기 때문에 시신경 보호 목적으로 0.15% brimonidine tartrate (Alphagan-P®; Allergan Korea Ltd.) 2회/일을 추가로 처방하였다.
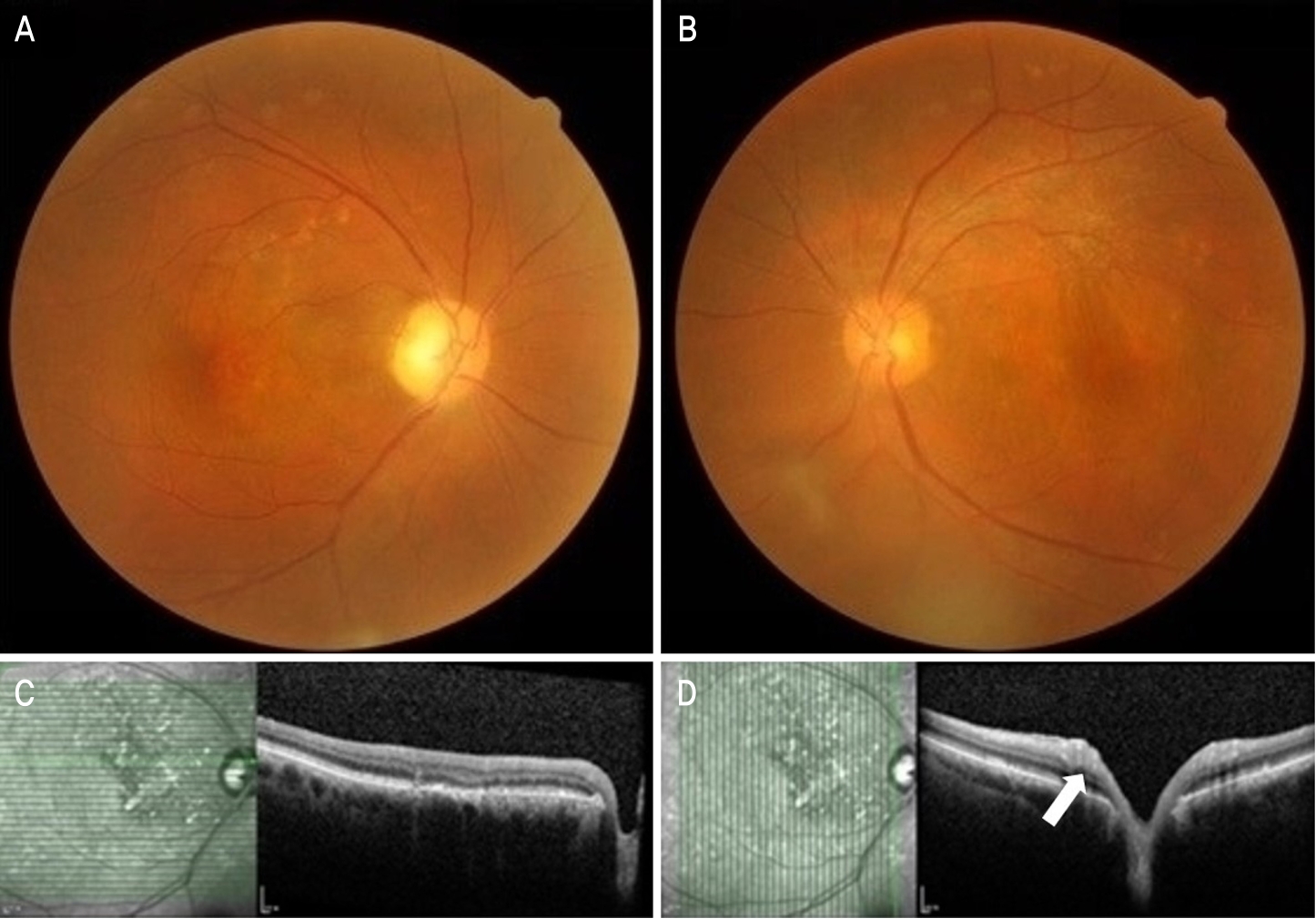
Fundus photography and optical coherence tomography (OCT) at 4 weeks after initial treatment. Fundus photography shows increased disc cupping and improved disc edema in right eye (A, B). Decreased thickness of the retinal nerve fiber layer and ganglion cell-inner plexiform layer (white arrow) are shown in OCT at 4 weeks after oral albendazole and prednisolone (C, D).
치료 시작 3개월 후 우안 교정시력은 0.15로 큰 호전을 보이지 않았다. 안저검사에서 우안 유리체 혼탁의 호전을 보였고 유두함몰은 큰 변화 없이 유지되었다(Fig. 4). 이후 약물은 경구 프레드니솔론을 20 mg 1회/일로 유지하며, 스테로이드 안약은 1% prednisolone 4회/일에서 0.5% loteprednol etabonate (Lotepro®; Hanlim Pharm. Co., Ltd, Seoul, Korea) 4회/일로 변경하였으며 이외 점안액은 유지하였다. 치료 시작 4개월 후 내원시 우안 시력은 0.125였으며, 세극등현미경검사에서 전방과 유리체 내의 염증세포는 관찰되지 않았다. 안저검사에서 우안 유리체 염증은 보이지 않았고 유두함몰이 관찰되었다. 시야검사의 pattern deviation에서 초진 시에 비해 우안 중심시야 결손의 진행이 확인되었다(Fig. 4). 경구 프레드니솔론은 2주 단위로 10 mg/일씩 감량한 후 중단하였으며, 점안액은 0.15% brimonidine tartrate 2회/일만 유지하고 이외 점안액은 모두 중단한 후 경과 관찰 중이다.

Widefield fundus photography at 3 months, and visual field examination at 4 months after initial treatment. Widefield fundus photography shows improved vitreous opacity and disc cupping (A). Visual field examination reveals an aggravated central visual defect compared to the initial presentation in right eye (B).
고 찰
눈개회충증의 임상 양상은 후극부 육아종(posterior pole granuloma), 주변부 육아종(peripheral granuloma), 선충성 안내염(nematode endophthalmitis), 비전형적 양상(atypical presentations)의 4가지로 분류할 수 있다[4]. 비전형적 양상으로는 시신경유두의 염증 및 부종, 망막 밑으로 움직이는 개회충, 전반적 맥락망막염이 보고된 바 있다[5-7]. 이러한 비전형 양상으로 눈개회충증에 의해 시신경유두의 염증 및 부종의 형태로 발생한 증례가 국내에 보고된 적은 이번이 처음이다.
Choi et al [8]의 연구에서 상대구심동공운동장애를 동반한 급격한 시력 또는 시야의 장애를 보이는 급성 시신경병증의 양상, 혈청학적 검사상 Toxocara canis IgG 역가 양성, 그리고 허혈시신경병증, 망막혈관폐쇄, 기타 자가면역질환, 염증성질환, 감염성질환 등 시신경병증을 일으킬 수 있는 이외 질환들이 배제될 때 눈개회충증에 의한 시신경병증(toxocara optic neuropathy)을 진단하였다. 그리고 비대칭적이거나 부채꼴 모양의 시신경유두 부종과 함께 유두주위 병변이 보일 경우 눈개회충증에 의한 시신경병증의 진단에 임상적으로 중요한 단서가 될 수 있음을 보고한 바 있다[8]. 본 증례는 전방과 유리체의 염증과 포도막염이 동반되면서 국소 시신경 부종 및 시신경 주변으로 국소망막 침윤 소견이 관찰되었으며 Toxocara canis IgG 정성검사 양성 소견이 관찰되었고, 생간 섭취의 식이습관이 있어 눈개회충증이 단안 시신경병증의 비전형적인 형태로 나타난 것으로 판단하 치료하였다. 고령의 나이 및 임상양상을 고려하였을 때 비동맥염성 앞허혈시신경병증의 배제가 필요하나, 비동맥염성 앞허혈시신경병증의 경우 일반적으로 시력저하와 비슷한 정도의 색각저하가 보이는 경우가 많으나 환자는 색각검사상 정상 소견을 보였다. 그리고 비동맥염성 앞허혈시신경병증에서 시신경유두 부종이 대개 전반적으로 나타나는 것에 비해 환자는 이측부가 심한 양상의 비대칭적 부종이 관찰되었으며, 고혈압, 당뇨 등 전신질환의 과거력이 없는 점에서 부합하지 않았고, 생간 섭취의 식이습관이 있어 눈개회충증에 보다 부합한 것으로 판단하였다.
눈개회충증의 치료에서 스테로이드의 사용은 표준화되어 있으나, 구충제의 효능에 대해서는 정립되어 있지 않다[9]. 그러나 Ahn et al [2]의 연구에 따르면 눈개회충증에서 알벤다졸과 경구 프레드니솔론 병합요법이 스테로이드 단독용법에 비해 6개월간 재발률이 유의미하게 낮음이 보고되었고, 따라서 본 증례에서도 알벤다졸과 경구 프레드니솔론 병합요법을 시행하였다. 진단 및 초기 치료가 늦어져 병합요법 4개월 후 우안 나안시력 0.125로 초진 시 나안시력 0.4에 비하여 저하되었고, 이는 적절한 치료에도 발생한 비가역적인 시신경 손상에 의한 것으로 생각되었다.
본 연구에서는 Toxocara IgG에 대한 정성 분석만 시행하였으며 titer를 확인하지 못 하였고, IgG에 대한 정량 검사 및 혈청 IgE 검사를 시행하지 못해 질병의 활성도와의 연관성을 확인하지 못한 것이 한계점으로 남아있다. 결론적으로 시신경염이 의심되는 환자에서 전방, 유리체의 염증과 포도막염이 동반되어 나타나는 경우 눈개회충증이 비전형적인 형태로 발현될 수 있으며 진단이 늦어질 경우 비가역적인 시신경 손상으로 나쁜 예후를 보일 수 있는 바 초기부터 개회충증 감염을 포함한 여러 감염성 질환의 가능성을 고려하여야 하며, 의심될 경우 적극적인 검사 및 치료를 요한다.
Notes
The authors have no conflicts to disclose.