공막렌즈의 특징과 환자 선택
Characteristics of Scleral Lenses and Patient Selection
Article information
Abstract
공막렌즈는 각막이 아닌 공막에 지지하여 각막 이상이나 안구표면질환이 있는 경우 시력을 개선시키고 각막에 수분을 공급하여 안구 표면질환의 치료에 도움을 준다. 공막렌즈 재질의 개선, 전안부 영상 장비의 발전 등으로 공막렌즈의 처방 비율은 늘어나고 있다. 공막렌즈를 성공적으로 처방하기 위해서 공막렌즈의 구조와 원리를 이해하고 적절한 환자를 선택해야 한다. 공막렌즈의 절대적인 금기는 없으나 주의가 필요한 환자들에게는 정기적인 경과관찰을 추천한다.
Trans Abstract
Scleral lenses lies on the sclera, not the cornea, and help to improve vision in cases of irregular cornea or ocular surface diseases, and to treat ocular surface diseases with moisture to the cornea. The fitting rate of scleral lenses is increasing due to improvements in scleral lens materials and advancements in anterior segment imaging equipment. In order to successfully fit scleral lenses, it needs to understand the structure and principles of scleral lenses and select appropriate patients. There is no absolute contraindication of scleral lenses, but regular follow‐up is recommended for patients who require caution.
서 론
공막렌즈는 윤부를 포함한 각막과 접촉이 없고 공막과 결막의 지지를 받는 콘택트렌즈를 말한다. 공막렌즈는 각막이 아닌 공막에 지지함으로 각막형태에 이상이 있는 경우에도 착용 가능하며 시력을 개선시킬 수 있고 렌즈 후면과 각막 앞면 사이 보유 눈물층(tear reservoir)이 있어 안구 표면을 보호하는 데 효과적이다. 공막렌즈의 첫 사용은 19세기에 유리로 만들어진 공막렌즈에 이어서 폴리메틸메타크릴레이트(poly[methyl methacrylate], PMMA)로 만들어진 공막렌즈가 개발되었으나 산소투과성이 떨어져 사용이 제한되었다. 이후 1983년 rigid gas‐permeable (RGP) 재질의 공막렌즈가 개발되면서 산소투과율을 증가시켜 합병증이 감소하였고[1] 전안부 광간섭단층영상이나 각공막지형도와 같은 영상 기기들의 발전으로 공막렌즈 처방이 증가하고 있다. 공막렌즈 처방 비율은 2011년 이후 크게 증가하였으며 2019년에는 2.3%에 도달하였다고 보고하였다[2]. 본 논문에서는 공막렌즈의 전반적인 특징과 적절한 환자 선택에 대해 알아보고자 한다.
공막렌즈의 특징
구조 및 원리
공막렌즈는 윤부를 포함한 각막 전체와 볼트(vault)를 형성하여 접촉이 없고 공막과 결막에 지지한다(Fig. 1). 각막의 모양에 상관없이 새로운 매끈한 표면을 만들어 주고 렌즈의 뒷면과 각막 표면 사이에 보유 눈물층이 존재하기 때문에 시력 개선에 큰 효과가 있고 각막에 지속적으로 수분을 공급해줄 수 있다. 또한 신경 분포가 적은 공막에 지지하여 이물감이 적고 착용감이 우수하다.
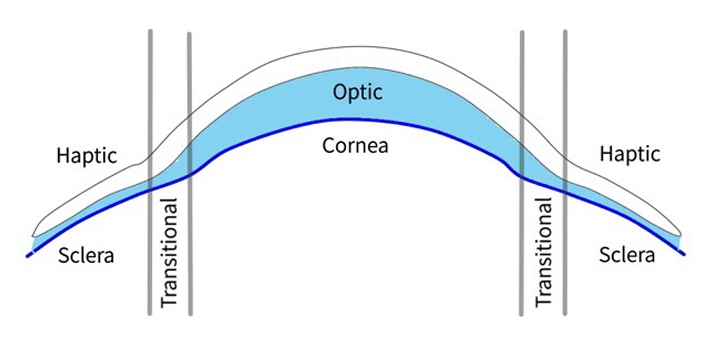
The design and structure of scleral lens.
공막렌즈는 보통 중심의 광학부(optic zone), 지지대인 공막부(landing or haptic zone), 두 부위를 연결하는 이행부(transition zone)로 구성되어 있다(Fig. 1) [3]. 광학부는 굴절값을 교정하는 가장 중앙 부위로 광학부의 전면은 난시나 비구면도, 고위수차 등을 줄이도록 제조될 수 있다[4,5]. 이행부는 여러 커브로 구성되며 곡률 또는 접선 각도를 변경하여 렌즈의 시상 높이를 만들어주고 주변부각막과 윤부의 보유눈물층 깊이를 조절할 수 있다. 공막부는 렌즈의 밀봉(seal off), 압착(suction), 중심잡기(centration), 공막눌림(compression) 등에 관여하며 공막이 눌리는 것을 최소화하고 렌즈 무게가 고르게 분포할 수 있도록 조절해야 한다[6‐9].
분류
Scleral Lens Education Society에서는 다양한 공막렌즈를 지지되는 부위에 따라서 각공막렌즈(corenal‐scleral/semi‐scleral, 12.5‐15 mm), 미니공막렌즈(mini‐scleral, 15‐18 mm), 공막렌즈(large scleral, 18‐25 mm) 등으로 분류하였다[10]. 각 공막렌즈는 공막렌즈보다 눈물 교환은 잘 이뤄지나 보유 눈물층이 적어 안구표면질환 치료 효과는 떨어진다. 하지만 직경이 작아 결막낭 길이가 짧거나 결막붙음증이 있는 경우 적합할 수 있다.
환자 선택
적응증
공막렌즈의 주요 적응증은 불규칙한 각막에서 시력 개선, 안구표면질환의 치료, 굴절 이상 교정, 스포츠 또는 미용 목적 등이 있다. 2020년 Scleral Lenses in Current Ophthalmic Practice (SCOPE) 연구에 따르면 공막렌즈 처방의 84%는 불규칙한 각막, 10%는 안구표면질환, 2%는 굴절 이상이었다고 보고하였다[11].
각막 이상 환자의 시력 개선
공막렌즈는 각막이 아닌 공막에 지지하기 때문에 각막의 모양에 영향을 받지 않아 불규칙한 각막에서 가장 많이 사용되고 있다. 원추각막, 투명각막가장자리변성, 공모양각막 등의 각막확장질환, 각막 이식 후의 난시, 굴절교정 수술 후 발생한 의인성 각막확장증이나 각막 혼탁 등에서 성공적으로 착용 가능하게 하고 시력을 개선시켜 준다(Fig. 2).
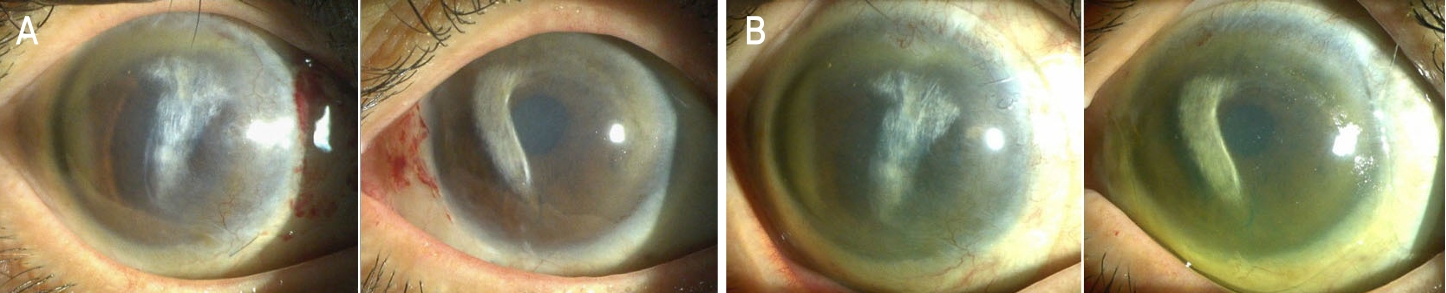
Scleral lens prescription for patients with irregualr cornea. (A) Slit‐lamp photographs of a patient with cental corneal opacities, neovascularization and severe irregular astigmatism. (B) Successful fitting of scleral lens. The best corrected visual acuity improved from count finger before wearing the scleral lens to 0.2 after wearing the scleral lens.
Baran et al [12]은 원추각막, 투명각막가장자리변성, 굴절 수술 후 각막확장증을 포함한 89안을 대상으로 Prosthetic Replacement of the Ocular Surface Ecosystem (PROSE) 공막렌즈(BostonSight®, Needham, MA, USA)를 시도하였을 때 모두 성공적으로 착용하였고 시력은 20/70에서 20/25로 향상되었다고 보고하였다. PROSE 공막렌즈를 착용한 36명의 원추각막 환자와 각막확장증으로 각막 이식술을 받은 37명의 환자를 비교하였을 때 공막렌즈 착용 그룹에서 더 우수하고 빠른 시력 회복을 보였다고 하였다[13]. 또한 급성 각막수종이 있는 원추각막, 투명각막가장자리변성, 각막수종이 있는 공모양각막 환자에서도 성공적으로 공막렌즈 착용이 가능하였으며 시력이 개선됨을 확인하였다[14‐16]. 또한 각막 흉터나 이영양증이 있는 경우도 공막렌즈 착용 전보다 후에 유의하게 시력이 개선되었다[17].
심한 안구표면질환의 치료
공막렌즈는 gas‐permeable 재질로 산소투과도를 높이고 눈에 안정적으로 위치하며 각막에 지속적으로 수분을 공급해주며 눈꺼풀테나 눈깜빡임에 대한 마찰을 차단하여 여러 안구표면질환의 치료와 시력 개선에도 효과적이다. 스티븐스존슨 증후군, 독성표피괴사용해, 화학 화상 등 각막줄기세포결핍, 쇼그렌증후군, 이식편대숙주질환, 방사선 조사 등의 눈물샘 손상으로 인한 심한 안구건조증, 지속각막상피결손, 신경영양각막병증 등에서 약물 치료 등으로 호전되지 않을 때 공막렌즈를 시도해볼 수 있다(Fig. 3).

Scleral lens prescription for patients with ocular surface disease. (A) Slit‐lamp photographs of a patient with chronic Stevens‐Johnson syndrome (SJS). She had conjunctial scarring and cicatrization, corneal scarring, neovascularization, and lid margin keratinization. (B) Fluorescein‐stained cornea showed punctate epithelial erosion. (C) Successful fitting of scleral lens for patients with chronic SJS.
스티븐스존슨 증후군, 독성표피괴사용해가 있는 환자에서 PROSE 렌즈를 착용하고 시력과 주관적인 증상이 크게 호전되었다고 보고하였다[18,19]. 그리고 만성 이식편대숙주병 환자에서 PROSE 렌즈를 착용하였을 때 98%에서 시력이 개선되었고 75%에서 지속 각막상피결손이 회복되었다는 연구가 있다[20]. 노출각막병증이나 신경영양각막병증으로 인한 지속각막상피결손에서도 PROSE 렌즈가 시력 개선과 각막재상피화를 달성하였다[21‐23]. 공막렌즈는 쇼그렌증후군이나 심한 건성안 환자에서도 건성안 증상과 징후가 좋아지고 잘 적응하였으며 합병증이 거의 없었다고 밝히고 있다[24,25].
굴절 이상
무수정체증이나 고도근시, 고도난시 등의 굴절 이상을 교정하는 데도 이용할 수 있다. Alipur and Hosseini [26]는 외상으로 인한 홍채각막 손상과 무수정체증 환자 8명에서 미니공막렌즈가 시력을 크게 개선시켰으며 보통 편안한 하루 평균 착용 시간은 11.6시간이었다고 보고하였다. 고도근시나 고도난시 등의 굴절 이상을 교정하는 데에 있어 공막렌즈는 각막 RGP 렌즈에 적응을 못하거나 불규칙 난시가 있는 환자에게 국한되었다[27].
상대적 금기 사항
공막렌즈 착용의 절대적인 금기로 알려진 것은 없다. 공막렌즈 착용에 주의가 필요하거나 상대적으로 금기가 되는 사항들은 각막 내피에 이상이 있거나 녹내장이 있는 경우, 그리고 수면 착용이 있다.
각막내피세포 이상
각막내피세포의 감소는 연령, 당뇨, 콘택트렌즈 착용, 안과 수술이나 건성안과 관련 있다고 알려져 있다. 콘택트렌즈 사용이 각막내피세포 밀도에 미치는 영향은 연구에 따라 차이가 있다. Hollingsworth and Efron [28]은 RGP 렌즈 착용이 각막내피세포 밀도에 영향을 주지 않는다고 보고했고 중앙 각막의 내피세포 밀도 감소는 실제로 세포가 손실되기보다 중앙에서 주변 각막으로 재배치된 것이라는 연구도 있다[29].
공막렌즈 착용이 각막내피세포에 미치는 영향을 보고한 연구는 거의 없다. 하지만 각막내피세포의 밀도가 떨어져 있거나 변동계수가 증가된 경우 공막렌즈 착용으로 인한 각막 부종 가능성이 있어 공막렌즈 착용 전 내피세포를 평가하는 것이 중요하겠다[30‐32].
녹내장
공막렌즈 처방은 녹내장 환자에서 주의가 필요하다. 공막렌즈는 공막 위의 결막에 지지하므로 방수 유출을 방해할 수 있다는 가설들이 있다. 여러 연구에서 공막렌즈를 단기간 착용 전과 후에 안압을 비교하였는데 증가하였다는 보고와 유의한 차이가 없었다는 보고들이 있어 아직 결론을 내리기는 어렵다. 한 연구에서는 공막렌즈 8시간 착용 후 안압이 평균 5.8 mmHg 상승했다는 보고하고 있지만[33] 대부분의 연구는 공막렌즈 단기 착용 후 안압 변화는 미미했다고 보고하고 있다[34‐37]. Kramer et al [38]은 공막렌즈 착용 전과 1개월과 6개월 후 안압은 증가하는 경향이었으나 유의미하지 않았다고 보고하였다. 또한 방수 유출 장치가 삽입되어 있는 경우 공막렌즈의 금기는 아니지만 마찰이 일어나지 않게 주의해야 한다[39,40]. 녹내장 위험이 있는 경우 공막렌즈 착용 중 정기적으로 안압을 평가하는 것이 도움이 되겠다.
결 론
공막렌즈는 각막 이상이나 안구표면질환이 있는 경우 시력을 개선시키고 각막에 수분을 공급하여 안구표면질환의 치료에 도움을 주며 각막 수술을 지연시킬 수도 있다. 공막렌즈 재질의 개선, 전안부 영상 장비의 발전 등으로 공막렌즈의 처방 비율과 적응증은 늘어나고 있다. 하지만 각막내피세포 이상이나 녹내장이 있는 경우 각막내피세포와 안압을 정기적으로 경과관찰해야 하겠다.
Notes
The author has no conflicts to disclose.
This research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number: HI22C071800).