소아 환자에서 녹색광 레이저 포인터로 인해 발생한 비전형적 절박황반원공을 유리체절제술로 치료한 1예
A Case of Green Laser Pointer-induced Atypical Impending Macular Hole Treated with Vitrectomy in a Pediatric Patient
Article information
Abstract
목적
소아 환자에서 녹색광 레이저 포인터가 눈에 조사된 후 발생한 비전형적 절박황반원공을 유리체절제술로 치료한 증례를 경험하여 이를 보고하고자 한다.
증례요약
13세 여자 환자가 녹색광 레이저 포인터를 눈에 조사한 후 발생한 우안의 시력저하 및 상측 시야결손을 주소로 내원하였다. 수상 당일 우안의 교정시력은 0.1이었고 광각안저촬영 및 빛간섭단층촬영에서 중심와를 침범한 망막앞출혈과 내경계막하출혈이 확인되었다. 특별한 치료 없이 경과관찰 하던 중 수상 후 4개월째 빛간섭단층촬영에서 망막앞출혈과 내경계막하출혈은 소실되었으나 새롭게 발생한 비전형적 절박황반원공이 관찰되었다. 내경계막이 원공을 덮은 채로 보존되어 원공의 자연폐쇄를 기대하고 경과관찰을 시행하였으나 수상 후 8개월째 빛간섭단층촬영에서 황반원공의 기저직경이 증가된 소견을 보였다. 이에 우안 유리체절제술, 내경계막제거술 및 유리체강 내 과불화프로판가스 주입술을 시행하였으며, 수술 후 1개월째 빛간섭단층촬영에서 황반원공은 해부학적으로 폐쇄된 소견이 관찰되었고 교정시력은 0.8로 회복되었다.
결론
소아 환자에서 녹색광 레이저 포인터가 눈에 조사된 후 발생한 망막의 출혈은 자연적으로 흡수될 수 있으나 이후 황반원공이 발생할 수 있다. 이러한 절박황반원공에 대해 유리체절제술을 이용한 수술적 치료로 효과적인 해부학적 폐쇄 및 시력의 호전을 이룰 수 있다.
Trans Abstract
Purpose
To report a case of atypical impending macular hole induced by green laser pointer in a pediatric patient treated with vitrectomy.
Case summary
A 13-year-old patient visited our clinic complaining of decreased visual acuity and upper visual field defect in the right eye after exposure to a green laser pointer. Her best corrected visual acuity was 20/200 in the right eye. Ultra-widefield fundus photography and optical coherence tomography showed pre-retinal hemorrhage and sub-internal limiting membrane hemorrhage involving the fovea. After 4 months of follow-up, the retinal hemorrhage was spontaneously resolved, however, atypical impending macular hole with intact overlying internal limiting membrane was observed on optical coherence tomography in the right eye. Regular follow-up was performed for spontaneous macular hole closure. After 8 months of follow-up, the base diameter of the macular hole increased on optical coherence tomography, accordingly, pars plana vitrectomy, internal limiting membrane peeling, and intravitreal perfluoropropane gas injection were performed in the right eye. After 1 month of the surgery, the macular hole was successfully closed and the best corrected visual acuity was 20/25 in the right eye.
Conclusions
In pediatric patient, retinal hemorrhage can be caused by green laser pointer, which may be spontaneously resolved. However, delayed macular hole can occur, and surgical intervention might be helpful for successful anatomical closure and recovery of visual acuity.
눈은 400-1,400 nm 범위의 파장을 가지는 광학 방사선이 조직 깊숙이 침투할 수 있는 유일한 신체 기관이다. 또한 각막의 굴절력은 빛이 망막에 도달하기 전에 방사조도(W/cm2)를 최대 105배까지 기하급수적으로 증폭시킬 수 있다고 알려져 있는데[1], 이러한 특성 때문에 레이저 포인터가 망막에 조사되는 경우 망막에 손상이 발생할 가능성이 있다.
레이저 포인터로 인해 망막이 손상된 환자에 대한 여러 연구들이 보고되었으며 이 중 특히 소아의 놀이행동이 관련 있는 경우가 가장 많았다(96.1%) [2,3]. 본 증례에서도 환자가 녹색광 레이저 포인터를 가지고 놀던 중 실수로 눈에 조사한 후 발생한 시력저하로 병원에 내원하였으며, 이후 지연성으로 절박황반원공이 발생하였고 이에 대해 수술적 치료를 시행하여 성공적으로 원공을 폐쇄하고 시력이 개선된 증례를 경험하여 이를 소개하고자 한다.
증 례
13세 여자 환자가 레이저 포인터를 가지고 놀던 중 우안에 레이저를 조사한 후 발생한 우안의 시력저하 및 상측 시야결손을 주소로 내원하였다. 수상 당시 사용했던 레이저 포인터는 녹색광 레이저를 사용한 것으로, 적색광 레이저에 비해 파장이 더 짧은 특징을 가지고 있다(Fig. 1).

A green light-emitting portable laser pointer irradiated to the patient’s right eye.
내원 당시 우안의 나안시력은 0.02, 교정시력은 0.1이었으며 안압은 17 mmHg였다. 세극등 검사에서 전안부는 특이소견이 없었으나 안저검사에서 우안에 중심와를 침범한 망막앞출혈이 관찰되었고 빛간섭단층촬영에서는 내경계막하출혈이 확인되었다. 출혈의 자연흡수를 확인하기 위해 외래추적검사를 지속적으로 시행하였다. 수상 후 2개월째 안저검사에서 우안의 망막앞출혈 및 내경계막하출혈은 감소하였으며 최대교정시력은 0.5로 회복되었고, 빛간섭단층촬영에서는 우안 황반원공을 연속성이 보존된 내경계막이 덮고 있는 소견이 관찰되었다(Fig. 2A-D).

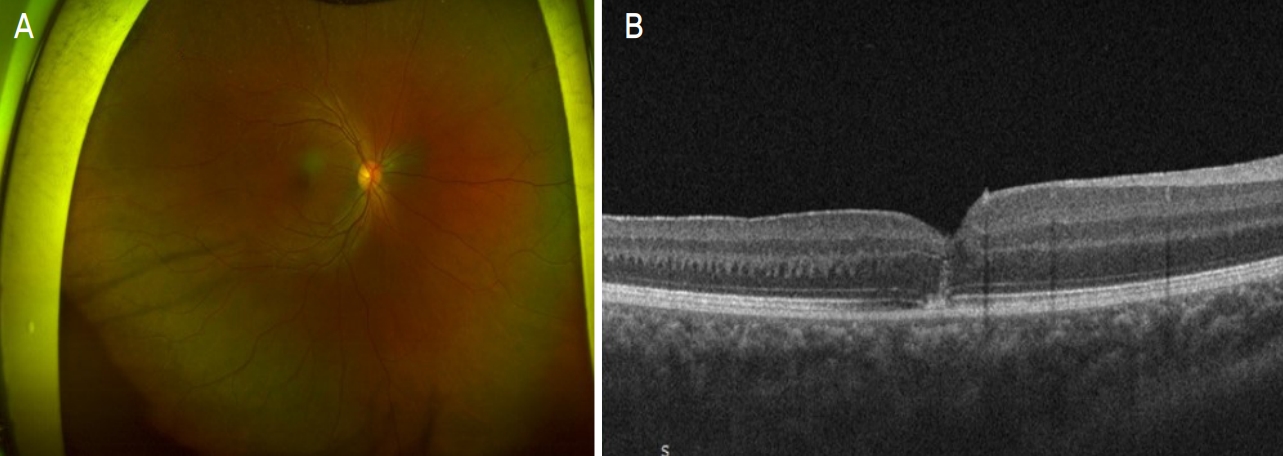
Ocular images of the patient’s right eye. (A) Ultra-widefield fundus photography (UWF) showed pre-retinal hemorrhage involving fovea (Baseline). (B) Optical coherence tomography (OCT) showed sub-internal limiting membrane (ILM) hemorrhage involving fovea (baseline). (C) UWF showed regression of pre-retinal hemorrhage (at 2 mo). (D) OCT showed regression of sub-ILM hemorrhage (at 2 mo). (E) UWF showed atypical impending macular hole (MH) with base diameter of 243 µm (at 4 mo). (F) OCT showed atypical impending MH (at 4 mo). (G) UWF showed enlargement of atypical impending MH (at 8 mo). (H) OCT showed an increase atypical impending MH with base diameter of 506 µm (at 8 mo).
수상 후 4개월째, 우안에 비전형적 절박황반원공이 새롭게 발생하였으며 최대교정시력은 0.4로 감소하였고, 빛간섭단층촬영에서 황반원공의 기저직경은 243 µm로 측정되었다. 내경계막이 보존되어 있어 황반원공의 자연호전을 기대하고 면밀한 경과관찰을 시행하였으나, 수상 후 8개월째 빛간섭단층촬영에서 황반원공의 기저직경이 506 µm로 증가된 소견이 관찰되었다(Fig. 2E-H). 이에 원공의 수술적 폐쇄를 시도하고자 우안 유리체절제술, 인도시아닌그린 색소 주입술 및 세척술, 내경계막 제거술 및 유리체강 내 과불화프로판(perflropropane, C3F8)가스 주입술을 시행한 후 2주일간 엎드린 자세를 유지하도록 하였다. 수술 후 1개월째 빛간섭단층촬영에서 우안의 황반원공이 해부학적으로 폐쇄된 소견이 관찰되었고 최대교정시력은 0.8로 호전되었다(Fig. 3).
Ocular images of the patient’s right eye after 1 month of vitrectomy. (A) Ultra-widefield fundus photography showed successfully closed macular hole (MH). (B) Optical coherence tomography showed successfully closed MH.
녹생광 레이저 포인터로 인해 망막이 수상된 당일부터 수술 후 1개월째까지의 경과를 빛간섭단층촬영을 통해 지속적으로 확인하였는데 수상 당일 내경계막하출혈이 관찰되었고(Fig. 4A), 수상 후 1.5개월째 및 2개월째 출혈이 점차 감소한 양상을 보였으며(Fig. 4B, C), 수상 후 2개월째 내경계막의 연속성이 유지된 상태로 대부분의 출혈이 소실된 소견이 관찰되었다(Fig. 4D). 수상 후 4개월째 새롭게 발생한 비전형적 절박황반원공이 관찰되었고(Fig. 4E), 수상 후 8개월째까지 내경계막의 연속성은 유지되나 황반원공의 기저직경이 점점 증가하는 소견을 보였다(Fig. 4F-H). 우안 유리체절제술을 시행하고 1개월 후 황반원공이 폐쇄된 소견이 확인되었다(Fig. 4I).

Serial follow-up optical coherence tomography of the patient’s right eye. (A) At baseline, massive sub-internal limiting membrane (sub-ILM) hemorrhage occurred. (B) At 1 month and (C) at 1.5 months, sub-ILM hemorrhage gradually decreased. (D) At 2 months, sub-ILM hemorrhage decreased with intact overlying ILM. (E) Atypical impending macular hole (MH) occurred at 4 months. (F-H) MH diameter increased during at 5-8 months. (I) MH was successfully closed 1 month after vitrectomy.
고 찰
레이저로 인한 안구의 손상은 광응고, 광파괴 또는 광화학적 메커니즘에 의해 나타날 수 있다. 큰 에너지가 나노초(nanosecond) 이내에 망막에 도달하면 이온화가 일어나고, 마이크로초(microsecond)에서 몇 초 동안 지속되면 열 손상(photothermal)이 발생하며 10초 이상 지속되는 경우 광화학(photochemical) 효과가 발생한다[3]. 이러한 망막 조직의 손상 정도를 결정하는 요인에는 레이저 광원의 종류, 맥락막 색소침착 정도, 그리고 손상 부위가 있다[4]. 녹색광 레이저는 망막색소상피층의 멜라닌 색소에 에너지를 전달하여 망막색소상피층과 외망막층에 손상을 일으킨다[3].
2000년대 중반 국제전자기술위원회(International Electrochemical Commission)는 레이저의 안전성에 기반한 분류를 소개한 바 있는데 이는 현재 미국국가표준협회(American National Standards Institute)에서 제시하는 레이저 안전기준에 포함되어 있다. 레이저 포인터는 상기 레이저의 안정성 분류 중 3R에 해당하는데, 이는 실수로 눈에 노출되었을 시 최대허용노출치를 초과하지만 눈 부상 위험 낮은 것으로 정의한다[3]. 본 증례에서는 이러한 위험성이 낮은 레이저 포인터로 인해 망막에 손상이 발생하였는데, 레이저의 위험성에 대한 자각이 크지 않은 소아 환자가 레이저를 눈에 오랜 시간 지속적으로 노출시켰을 가능성을 생각해볼 수 있다[5]. 안구 적출이 예정된 안구에 저전력의 녹색광, 적색광 레이저 포인터를 각각 오랜 시간 조사한 후 망막의 손상을 비교한 연구에서 적색광 레이저 포인터는 망막의 손상을 일으키지 않은 반면 녹생광 레이저 포인터는 망막의 손상을 유발했다고 보고한 바 있는데, 이는 3R에 해당되더라도 특히 녹생광을 이용한 레이저 포인터의 경우 망막을 손상시킬 수 있다는 가능성을 뒷받침한다[6]. 따라서 이러한 위험성을 인지하고 레이저 포인터를 안전하게 사용하는 것이 중요하다고 할 수 있겠다.
다양한 레이저로 인해 발생한 외상성 황반원공에 대해 수술적 치료로 호전된 증례들이 보고된 바 있다. Ciulla and Topping [7]은 titanium-sapphire 레이저 손상으로 유발된 황반원공 환자에서 수술적 방법으로 치료한 환자를 처음으로 보고하였고 편평부 유리체 전절제술, 망막전막 박피술 시행 후 시력개선 및 중심암점의 크기가 작아지는 호전 증상을 보였다 Ben-Simon et al [8]은 neodymium-doped yttrium aluminum garnet (Nd:YAG) 레이저에 수상한 35세 환자를 대상으로 본 증례와 유사한 방법으로 치료를 시행하였는데, 편평부 유리체 절제술, 인도시아닌그린 색소 주입 및 세척술, 내경계막 박피술을 함께 시행하였다. 상기 환자에서는 두 차례의 유리체절제술을 시행하였는데 첫 번째 유리체절제술 시에는 내경계막 박피술을 시행하지 않았고 황반원공이 충분히 폐쇄되지 않았다. 이에 두 번째 수술에서 내경계막 박피술을 포함한 부분 유리체절제술을 시행하였고 이후 황반원공이 폐쇄되었는데, 내경계막 박피술을 동반한 수술적 치료가 효과적일 수 있음을 시사하였다.
반면 소아 환자의 외상성 황반원공에서 치료 없이 자연 호전된 보고들도 있다[9,10]. Chandra et al [11] 은 황반부 모세혈관확장증으로 인해 황반원공이 발생한 환자에서 원공 위에 내경계막 덮개가 남아 있는 경우 원공의 자연적인 폐쇄를 보여준 증례를 보고하였는데, 저자들은 내경계막이 주로 뮬러세포와 성상교세포의 기저막에 의해 형성되며, 이러한 세포들에 의한 ‘브릿징 메커니즘(bridging mechanism)’이 원공폐쇄를 촉진할 수 있다고 추측하였다. 또한, 황반원공의 수술적 치료법에서 동종 내경계막 피판을 원공에 이식하는 수술기법이 Michalewska et al [12]에 의해 소개되었고, 내경계막 피판으로 원공이 성공적으로 닫히게 되는 원리에 대해서 Shiode et al [13]이 다음과 같이 설명하고 있다. 먼저, 내경계막은 뮬러세포의 증식과 이동을 위한 지지체 역할을 한다. 활성화된 뮬러세포는 신경영양인자 및 basic fibroblast growth factor (bFGF)가 생성하는데, 이러한 물질들이 내경계막 자체에도 존재하며 원공에 위치한 내경계막이 신경영양인자와 bFGF를 원공 부위에 직접 공급할 수 있다. 즉, 이식된 내경계막 피판에 의해 유발된 뮬러세포의 신경영양인자 및 bFGF와 같은 체액성 인자가 황반원공의 폐쇄에 기여할 수 있음을 시사하였다. 본 증례에서도 빛간섭단층촬영에서 원공 위로 연속성이 보존된 내경계막이 덮개로 작용하여 원공의 자연적인 폐쇄를 유도하길 기대하였으나 황반원공의 기저직경이 점차 증가하였고, 이에 소아 환자에서 외상성 황반원공을 수술적인 방법으로 성공적으로 폐쇄한 기존 연구를 바탕으로 수술적 치료를 시도하였다[14].
소아 환자에서 녹색광 레이저 포인터로 인해 망막의 출혈이 발생하는 경우 이는 자연적으로 흡수될 수 있으나, 추후 지연성으로 황반원공이 발생할 수 있다. 따라서 이러한 환자가 내원 시 동반 가능한 합병증 및 수술적 치료의 가능성을 충분히 설명하고, 특히 수개월의 시간이 경과한 후에도 합병증이 발생할 가능성을 염두에 두고 지속적인 경과 관찰이 필요하며 수술적 치료를 통해 망막의 해부학적 개선과 시력의 회복을 기대해볼 수 있겠다.
Notes
The authors have no conflicts to disclose.