가시아메바 각막염의 임상적 진단과 치료
Diagnosis and Management of Acanthamoeba Keratitis
Article information
Abstract
가시아메바 각막염은 심한 경우 각막 혼탁을 남겨 영구적 시력저하를 야기할 수 있는 질환으로, 대부분 콘택트렌즈 착용과 관련되어 발생하는데, 최근 콘택트렌즈 사용자의 증가와 더불어 발생도 증가하고 있다. 눈에 보이는 소견에 비해 심한 통증, 방사각막신경염, 고리모양침윤이 비교적 특징적인 증상이나, 임상에서 비전형적인 증상을 보여 진단이 늦어지는 경우가 있다. 진단은 각막 검체에서 가시아메바 영양형이나 포낭을 확인하는 것이나, 현실적으로 사용하기 어려운 경우에는 임상 소견을 통해 빠른 진단과 치료를 시작하는 것이 예후에 중요하다. 본고에서는 사진을 통한 가시아메바 각막염의 다양한 임상 소견과 치료에 대해 알아보고자 한다.
Trans Abstract
Acanthamoeba keratitis (AK) is a vision-threatening corneal infection that most frequently affects contact lens wearers. Severe pain out of proportion to the corneal findings, radial keratoneuritis, and ring infiltration are relatively specific clinical manifestations of AK. The diagnosis of AK is challenging and it is often misdiagnosed because of atypical presentations. The definitive diagnosis of AK requires the presence of Acanthamoeba cysts or trophozoites in corneal lesions, and a high index of clinical suspicion is important for early diagnosis. In this review, we describe the clinical manifestations, including atypical findings, and management of AK.
가시아메바(Acanthamoeba)는 오염된 물과 토양에서 흔히 발견되는 원생동물로[1], 가시아메바 각막염(Acanthamoeba keratitis)은 대부분 콘택트렌즈 착용과 관련되어 발생하고, 진단 시기에 따라 예후가 다르기 때문에[2], 콘택트렌즈 착용자에서 증상 발현 시 의심하여 빠른 치료를 시작하는 것이 중요하다[3]. 가시아메바 각막염의 여러 가지 임상 소견을 중심으로 진단과 치료에 대해 알아보고자 한다.
본 론
임상소견
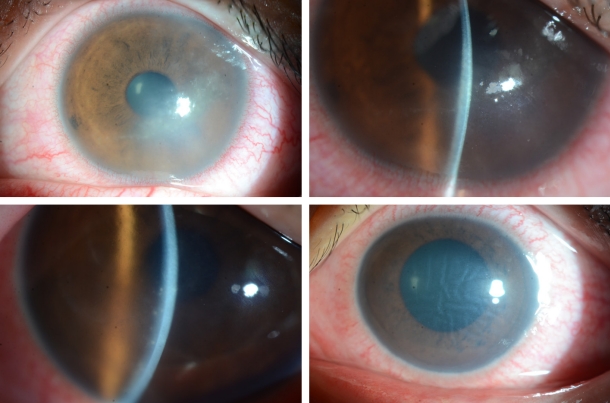
가시아메바 각막염은 대개 단안에 이환되나, 양안에 이환된 경우가 6.6%였다는 보고도 있다[4]. 특징적인 증상은 ‘눈 소견에 비해 심한 통증’으로, 가시아메바 영양형(trophozoites)이 각막신경세포 친화력이 있어 신경세포사멸이나 세포자멸사를 일으키기 때문에 생기나, 통증이 없는 경우도 있다[5]. 초기에 상피 병변에 국한될 경우 점모양각막병증(punctate keratopathy)이나 거짓가지모양(pseudodendrites)을 보이기도 하여(Fig. 1), 각막진무름이나 단순포진각막염으로 오진할 수 있다. 가시아메바가 신경세포 주변에 모여 염증을 유발하는 방사각막신경염(radial keratoneuritis)은 60% 이상에서 발견되며 비교적 특징적 소견으로 알려져 있어 임상적 진단에 도움을 주나(Fig. 2), 초기부터 관찰되지 않는 경우에 감별이 어려울 수 있다. 가시아메바가 점차 실질로 침투하여 심한 염증을 유발하면, 고리모양침윤(ring infiltration)이 나타난다(Fig. 3). 실질 염증이 심해지고, 각막후면 침착물(keratic precipitate)과 각막부종이 동반되면 내피염과 비슷한 양상으로 관찰되어 단순포진각막염으로 오진할 수 있다(Fig. 4) [6]. 안내 염증이 진행되는 경우, 홍채에도 영향을 주어 홍채위축이 진행되는 경우도 있고(Fig. 5), 이차 녹내장이 발병하는 경우도 있다. 가시아메바가 각막 주변부로 이동하여 공막을 침범하면 공막염이 나타나기도 한다.
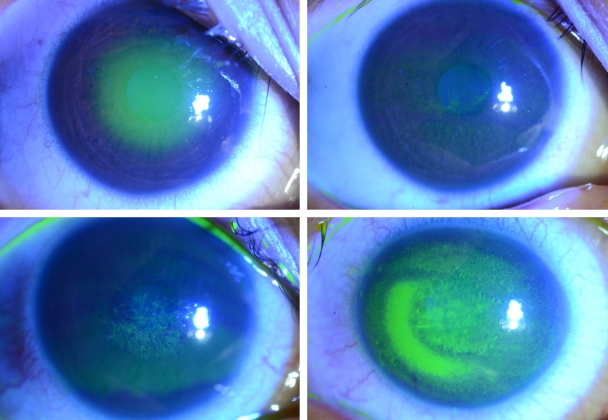
Slit-lamp photographs of early-stage Acanthamoeba keratitis and corneal epitheliopathy.
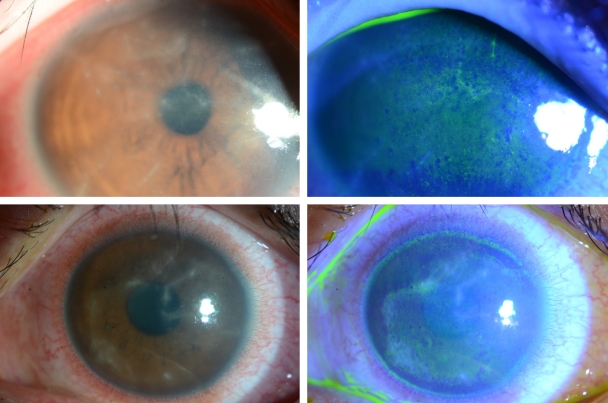
Slit-lamp photographs of epitheliitis and radial perineuritis.

Slit-lamp photographs of progression and healing of ring infiltration during the 5-month treatment.
Slit-lamp photographs of stromal infiltrates and endotheliitis mimicking herpes keratitis.
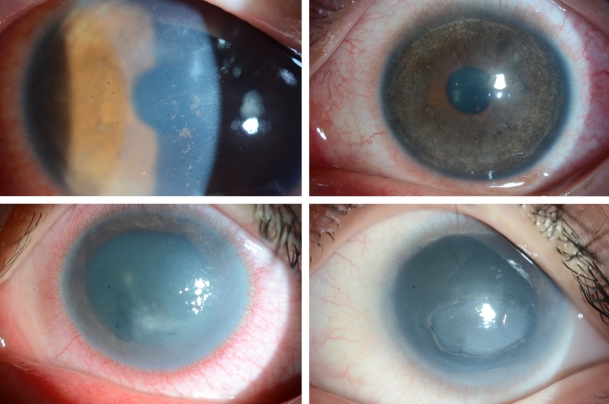
Slit-lamp photographs of uveitis due to Acanthamoeba keratitis, resulting in iris atrophy and aniridia.
진단
가시아메바 각막염의 진단은 염색, 배양, 조직검사를 통해 가시아메바 영양형(trophozoites)이나 포낭(cysts)을 확인 하는 것이나, 현실적으로 사용하기 어려운 경우도 있어 특징적인 임상 소견으로 진단하여 치료하는 것이 도움이 된다. 진단의 gold standard는 상피 손상이 심한 부위의 각막 상피를 긁어 배지에 접종하여 배양하는 것이며, 배지는 대장균이 도포된 비영양형 배지 Escherichia coli (E. coli)-seeded non-nutrient agar plate를 사용하여 가시아메바가 E. coli를 포식하고 이동한 길을 확인하는 것으로, 검출률은 60-76% 로 알려져 있다[5]. 배양으로 가시아메바를 검출하려면 1-2주가 걸릴 수 있어, Haematoxylin and Eosin, Gram, Giemsa, methenamine silver, periodic acid-Schiff, calcofluor white, acridine orange 등 여러 염색법을 이용한 슬라이드 관찰이 도움이 될 수 있다.
동일초점현미경(confocal microscopy)은 빠르고, 비침습적으로 가시아메바 포낭을 확인할 수 있는 방법으로 90% 이상의 민감도와 특이도를 보인다[7,8]. 동일초점현미경에서 가시아메바 포낭은 어두운 고리모양의 내벽과 경계가 뚜렷한 밝은 외벽으로 둘러싸인 고반사의 핵을 가진 “signet-ring” 모양으로 관찰되는 이중벽 포낭으로 관찰되나[9], 다른 염증 세포와 구별하기 어려운 경우도 있어 주의를 요하는데, 최근 한 연구에서 염증세포는 불규칙한 타원형으로 외벽이 없는 포낭과의 감별점을 제시하였다[7]. 그 외 중합효소연쇄 반응(polymerase chain reaction)은 85-90%의 민감도 및 특이도를 가지는 검사로 배양음성의 경우에도 양성을 보이는 경우도 있어 유용하나, 개체 사멸 후에도 양성을 보일 수 있어 질환의 활성도를 감별할 수는 없는 단점이 있다[10]. 치료에도 불구하고 지속되거나 재발되는 경우 조직생검을 통한 현미경적 검사를 고려해 볼 수 있다.
최근 진단에 전안부빛간섭단층촬영(anterior segment optical coherence tomography)을 이용하여 각막신경염이 고반사의 띠처럼 관찰되는 것을 보고한 경우도 있어 진단에 보조적으로 사용할 수 있겠다[11-13].
치료
가시아메바는 활발하게 증식하는 영양형(trophozoites)과 휴면 상태인 포낭(cyst)의 두 가지 형태로 존재하고, 포낭 시기에 이중의 포낭벽으로 둘러싸여 있어 오랫동안 생존할 수 있어 포낭을 박멸하는 데 치료 기간이 길어질 수 있다[14]. 현재까지 가시아메바 영양형과 포낭형 모두를 효과적으로 사멸시킨다고 알려진 것은 소독제로도 쓰이는 바이구아니드(biguanide) 계열의 약물인 0.02% polyhexamethylene biguanide (PHMB)와 0.02% chlorhexidine digluconate가 있으며, PHMB와 chlorhexidine 두 약제의 단독 치료를 비교한 randomized controlled trial에서 유의한 차이는 없었다[15]. Lee et al [16]의 이들 두 약제의 농도와 노출시간에 따른 각막 기질세포(keratocyte)의 세포사를 확인한 실험실 연구에서 PHMB가 더 독성이 있는 것을 확인한 바 있다. 또한 이들 약물을 장기간 사용 시 치료 과정에서 독성 각결막염이 생길 수 있어, 이와 관련된 충혈을 염두에 두고 환자에게 가능성을 설명할 수 있다. 대부분 임상에서 여러 약제를 복합적으로 사용하는 경우가 많으나, 복합 치료가 단독 치료에 비해 효과적이라는 근거는 없는 실정이다. 한 실험실 연구에서, 1% voriconazole이 가시아메바 영양형과 포낭형의 사멸에 1차 치료제로 알려진 chlorhexidine과 유사한 정도로 효과가 있으며, 세포독성은 적다고 하였고, 5% moxifloxacin도 포낭 형성 예방효과가 있어, 가시아메바 각막염 에서 복합 치료제로 고려할 수 있다[17]. 경구 voriconazole도 치료에 도움이 될 수 있어 치료 반응이 적은 환자에게 사용할 수 있다[18]. 기존 약제들이 장기 사용이 필요하나 안구 독성이 있는 점을 고려하여, 2016년 미국 Food and Drug Administration이 기존에 리슈만편모충증 치료제로 사용되던 경구 miltefosine (hexadecylphosphocholine; Impavido, Profounda, Inc.)을 가시아메바 치료를 위한 희귀의약품으로 인정한 후 이의 보조적 치료의 효과를 보고한 연구들이 있고[19,20], 경구약제의 위장장애, 간독성, 신독성을 고려하여 최근에 점안제로 투여한 연구에서 심한 가시아메바 각막염에서 miltefosine 점안액 단독 치료는 효과가 없는 것으로 보고되어 추가적 연구가 필요한 상태이다[21,22].
가시아메바는 Pseudomonas aeruginosa, Fusarium spp. 같은 다른 병원균을 세포 내 운반하여 세균이나 진균의 중복감염이 보고되기도 하여, 치료에 반응이 적을 때 중복감염을 고려해야 한다.
가시아메바 각막염에서 심한 염증을 동반하여 항아메바 약물과 더불어 스테로이드가 사용되기도 한다. 하지만 항아메바약물 시작 전 스테로이드의 사용은 진단 지연, 최종 시력저하, 각막이식이 필요한 심한 단계로 진행하는 나쁜 예후에 유의한 영향을 줄 수 있어[4,23], 가시아메바 진단이 의심될 경우에는 스테로이드 사용은 항아메바 약물이 시작된 후, 감염 징후가 조절되는 것을 확인하며 사용하는 것이 권장된다.
가시아메바 치료는 약물 치료가 일차적으로 시도되지만, 감염이 조절되지 않는 경우, 각막 혼탁으로 시력저하가 있는 경우 각막이식을 시행한다. 각막교차결합술과 냉동 치료도 보조적 치료적 방법으로 시도되기도 하였으나, 효과가 제한적으로 보고되었다[24,25].
결 론
최근 가시아메바 각막염 194안을 대상으로 한 해외 보고에서 고리모양침윤이나 공막염을 동반한 심한 염증, 항아메바 치료 전 스테로이드 투여, 진단 전 증상 기간(37일 초과), 34세 이상 연령이 나쁜 예후와 관련이 있고, 항아메바 치료 전 스테로이드 사용과 헤르페스 각막염 치료력이 심한 염증과 관련되었다고 보고하였다[26]. 또한 진단 시 상피 병변과 방사각막신경염만 관찰된 경우에는 시력 예후가 좋다는 보고가 있다[27,28]. 비전형적인 각막 병변이 관찰되는 환자에서 콘택트렌즈 사용력을 반드시 확인하고, 의심을 하여 빠른 진단과 치료를 시작하는 것이 예후에 무엇보다 중요하다.
가시아메바 각막염이 대부분 콘택트렌즈와 관련하여 발생하고, 최근 소아의 근시 조절을 위해 사용량이 증가하면서 각막굴절교정렌즈(orthokeratology lens)와 관련된 가시아메바 감염도 보고되고 있다[29,30]. 콘택트렌즈 사용자나 보호자들에게 보관용기를 철저히 소독하고, 오염된 물에 접촉, 수돗물에 접촉하지 않는 등 위생에 대한 교육을 하는 것이 가시아메바 각막염을 예방하는 데 중요하겠다[3,31]. 또한 가시아메바 각막염 후 각막 혼탁으로 시력과 관련된 삶의 질이 저하될 수 있어[32], 각막 혼탁이 생겼을 때 가스투과경성콘택트렌즈(rigid gas permeable contact lens)나 공막렌즈 등을 이용한 시력 재활을 위한 노력 및 지지도 중요하다.
Notes
The authors have no conflicts to disclose.