각막교정술(orthokeratology)은 근시 교정의 경우 주변부에 비해 평평하게 디자인된 gas permeable (GP, 경성 산소 투과) 렌즈를 이용하여 근시와 난시를 교정하는 방법으로, 근시 각막굴절교정수술과 유사하게 중심 각막을 편평하게 교정하여 각막굴절력을 감소시켜 결과적으로 굴절이상을 교정하게 된다[
1,
2]. 각막교정렌즈(Ortho-K)의 장점은 안경 착용에서 자유로워지며, 성장하면서 진행되는 근시의 진행 정도를 감소시킨다는 점이다. 정도의 차이는 있지만, 다양한 연구에서 렌즈 착용이 안구길이 증가를 대조군과 비교하여 감소시키는 것으로 알려져 있다[
3,
4]. 한 가지 고려해야할 점은 각막교정렌즈 착용 중지 후 근시의 진행인데, 안구 길이의 증가가 착용 때와 비교하면 빠르게 진행하지만 근시 진행 억제를 위한 다른 치료와 비교해서는 그 정도가 덜하고, 그동안 렌즈 착용에 의한 근시 진행 억제 효과를 고려하면 성공적인 조절 방법 중 한 가지로 고려된다[
5]. 성공적인 각막교정렌즈를 처방하기 위해서는 시술 전 몇 가지 필수적인 검사를 시행해야 하며, 이를 통해 교정 효과가 낮거나 적응이 되지 않는 경우 또는 착용 후 발생 가능한 문제를 미리 파악할 수 있다. 본고를 통해 시술 전 시행하는 검사와 그 의미에 대하여 알아보도록 하겠다.
본 론
Table 1에 나열한 시술 전 검사와 검사를 위한 기구는 일반적으로 GP렌즈 처방 시와 크게 다르지 않다. 환자의 굴절이상을 정확하게 파악하기 위하여 굴절교정검사를 시행하고, 각막굴절력을 파악하기 위하여 각막곡률계(keratometer)를 시행하게 된다. 각막지형도는 난시의 양과 축을 파악하는 데에 유용할 뿐만 아니라, 난시의 형태와 범위 그리고 불규칙 난시의 여부를 파악할 수 있어 다른 렌즈 처방과 달리 각막교정렌즈 처방에 필수적인 검사이다. 시술 전 각막 지형도는 이후 각막의 변화에 대한 정보를 제공하여 추적 관찰 시 렌즈와 눈의 관계를 파악하는 데에 중요하고, 시술 전 일부 렌즈에서 기본 파라미터로 사용하는 편심률(eccentricity, “e”)을 제공하며 “e”값이 너무 높거나 너무 낮은 경우(교정량은 “e”값에 비례하므로 특히 낮은 경우) 교정해야 할 굴절력이 크다면 그 효과가 제한적일 가능성이 높다. 세극등현미경검사를 시행할 때 플루레신형광염색을 통하여 각막표면 상태를 평가할 수 있고, 눈꺼풀, 결막 등을 관찰하여 마이봄샘염, 알레르기결막염, 눈썹위치이상 등을 평가해야 한다. 렌즈의 크기를 정하기 위해 white to white diameter와 horizontal visible iris diameter를 측정하는 것이 도움이 된다[
6,
7].
성공적인 렌즈 처방을 위해서는 효과가 적을 것으로 예상되거나 중심이탈 등 합병증이 생길 가능성이 높은 후보자를 미리 선별하여 다른 종류의 굴절교정 방법을 권유 또는 이에 대한 이해를 통하여 현실적인 기대치를 재설정하거나 추후 발생할 문제점을 미리 설명하여 렌즈 디자인 교환이나 수정이 필요할 가능성에 대하여 미리 설명하는 것이 바람직하다. 가정 먼저 고려해야 할 것이 근시와 난시의 정도인데 근시는 각막굴절력과 “e” 값에 따라 그 교정량이 제한적이므로 일반적으로 근시의 정도가 심할수록 효과가 제한적일 수 있고 난시는 절대치 난시의 위치(
Fig. 1)에 따라 교정량과 렌즈의 중심잡기에 영향을 미치게 된다. 일반적으로 제조사에 따라 Food and Drug Administration (FDA)에서 권고하고 있는 허용 기준은
Table 2와 같으며 렌즈는 초심자의 경우 낮은 도수의 근시와 난시가 없거나 또는 약간의 with-the-rule (WTR) 난시가 있는 굴절이상을 대상으로 시작해 보는 것을 추천한다[
5,
6,
8].
난시용 각막교정렌즈(Toric Ortho-K)와 고도근시용 각막교정렌즈의 개발과 더불어 교정 가능한 굴절이상의 범위와 중심잡기가 개선되고 있으나, 일반적으로 근시는 4.5 diopters (D) 이내, WTR 난시는 1.5 D 이내, against-the-rule 난시는 0.75 D 이내, 난시가 각막중심에 분포하고 있는 경우, 렌즈 유발 난시가 0.5 D 이내, 그리고 정상 또는 조금 높은 “e” 값을 가지고 있는 경우 교정 효과가 더 우수하다(
Table 3). 저자의 경험에 비추어 보면 소아청소년에 비하여 성인의 경우 특히 업무량이나 야간운전이 많은 경우 약간의 중심 이탈이나 교정 이상에도 민감하게 반응하는 경우가 많아 더욱 주의를 요한다[
6,
7].
제조사마다 권고하는 방법에 따라 파라미터를 이용해서 렌즈를 착용한 후, 형광염색을 이용하여 렌즈의 상태를 파악하며
Fig. 2와 같은 기준으로 렌즈와 각막과의 상태를 판별하고, 그 결과에 따라 base curve를 조절하게 된다. Ortho-K렌즈는 형광염색패턴보다는 착용 후 각막지형도의 변화를 평가하는 것이 보다 중요하다[
6,
9].
각막지형도검사는 난시용 각막교정렌즈의 난시값을 결정할 때 사용할 수 있는데, 일부 렌즈에서는 정렬곡선(alignment curve)이 각막과 만나는 부분에서 가파른(steep) 축과 편평한(flat) 축의 elevation 차이를 수치로 계산해서 그 차이에 따라 렌즈의 난시 정도를 결정한다. 이때 각막지형도의 anetior elevation map을 유용하게 사용할 수 있다(
Fig. 3) [
10,
11].
결 론
성공적인 렌즈 맞춤을 위해서는 적절한 대상자를 선정하는 것이 가장 중요할 것으로 생각된다. 안과에 내원하는 다른 환자의 진료와 크게 다른 검사를 필요로 하지는 않으며, 각막지형도에서 가장 많은 정보를 얻을 수 있어 각막지형도의 정보를 정확하게 해석할 수 있어야 한다. 또한 협조도가 떨어지는 소아청소년 환자의 경우 미세한 움직임, 눈썹, 미숙한 검사자 등의 이유로 잘못된 정보를 제공하는 경우도 있어 이에 대한 반복 검사 또는 다른 기계 검사값과의 비교를 통해 이중 점검하는 과정이 필요하다.
Conflicts of interest
The authors have no conflicts to disclose.
Figure 1.
Corneal topographic finding. (A) Corneal astigmatism remains in the center. (B) Corneal astigmatism extends form limbus to limbus.
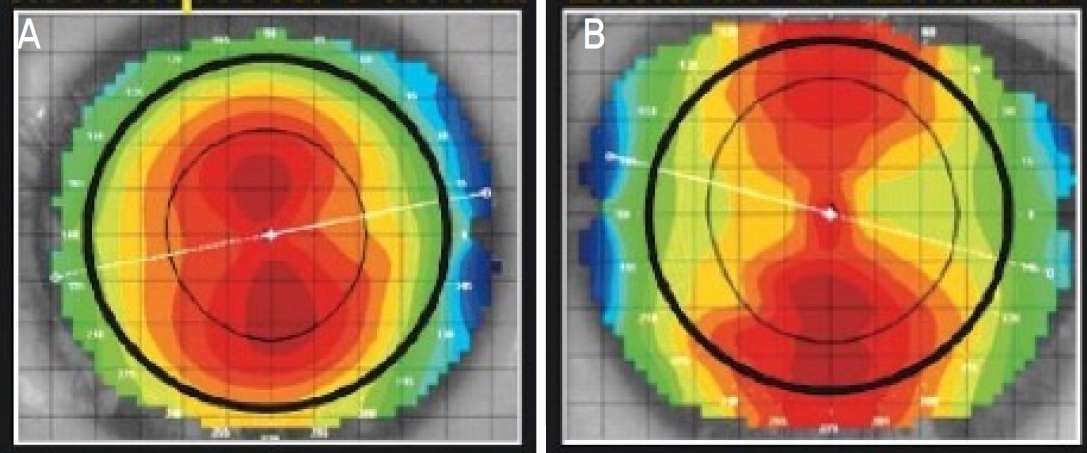
Figure 2.
Fluorescein pattern of tight or loose orthokeratology lens fitting.
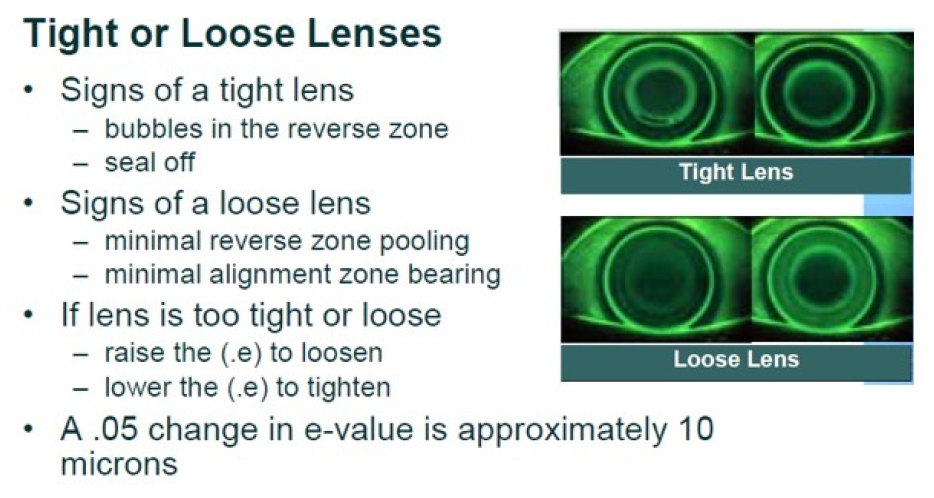
Figure 3.
Deternimation of toricity for initial orthokeratology lens fitting. D = diopters; RZD = return zone depth; LAZ = landing zone angle.
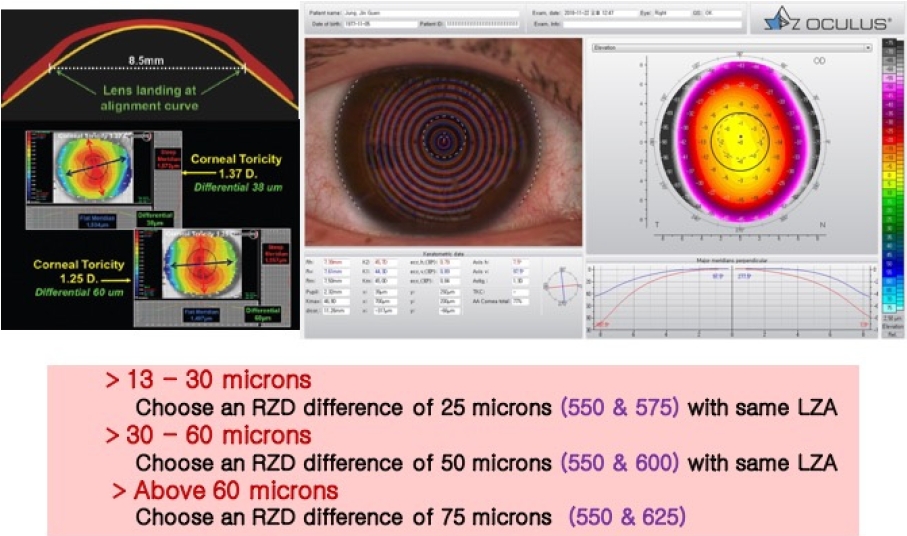
Table 1.
Pre-fitting examination and instruments required for orthokeratology lens prescription
|
Pre-fitting examination |
Instruments required/suggested |
|
-Refraction (with dilation) |
-Topographer (preferred) or keratometer (minimal) |
|
-Baseline topography (keratometry optional, but topography is a must) |
-Slit-lamp biomicrosope |
|
-Tear film analysis-Schirmer test, TBUT |
-Autorefractor, phoropter, or universial trial frame |
|
-Biomicoscopy |
-Visual acuity charts |
|
-WTW, HVID |
-Contrast sensitivity charts (maybe helpful to quantify visual acuity) |
Table 2.
United States FDA approval of orthokeratology contact lenses
|
FDA approval for corneal refractive therapy |
|
Up to -6.00 D of myopia |
|
Up to -1.75 D of astigmatism |
|
No age limitations |
|
FDA approval for vision shaping treatment |
|
-1.00 D to -5.00 D of myopia |
|
Up to -1.50 D of astigmatism |
|
No age limitations |
Table 3.
Various factors that affect favor clinical results
|
Good candidates |
Poor candidates |
|
Lower to moderate myopia (-4.5 D) |
K < 39.0 D or K > 48.0 D |
|
WTR ≤ 1.5 D |
ATR or oblique astigmatism > 0.75 D |
|
Lenticular astigmatism > 0.5 D ATR |
|
Limbus to limbus astigmatism |
|
Pupil size ≤ 6.0 mm in dim illumination |
Large pupil in normal illumination |
|
Normal, healthy cornea, lids & conjunctiva |
Active or recurrent ocular surface disease |
|
Normal tear break-up time |
|
Corneal “e” correlates with the refractive change required |
Low “e” corneas requiring high refractive change |
|
Non-habitual spectacle wearers |
|
SCL wears with end-of-day dryness |
|
Active sportspeople |
Prior history of poor compliance |
|
Unrealistic expectation |
REFERENCES
1) Nichols JJ, Marsich MM, Nguyen M, et al. Overnight orthokeratology. Optom Vis Sci 2000;77:252-9.


2) Haque S, Fonn D, Simpson T, Jones L. Corneal and epithelial thickness changes after 4 weeks of overnight corneal refractive therapy lens wear, measured with optical coherence tomography. Eye Contact Lens 2004;30:189-93.
3) Li SM, Kang MT, Wu SS, et al. Efficacy, Safety and acceptability of orthokeratology on slowing axial elongation in myopic children by meta-analysis. Curr Eye Res 2016;41:600-8.
5) Bullimore MA, Johnson LA. Overnight orthokeratology. Cont Lens Anterior Eye 2020;43:322-32.
6) Bennett ES, Henry VA. Clinical manual of contact lenses. 1st ed. Philadelphia: Lippincott Williams & Wilkins; 2000. p. 1-639.
7) Cho P, Cheung SW, Mountford J, White P. Good clinical practice in orthokeratology. Cont Lens Anterior Eye 2008;31:17-28.
8) Gu T, Gong B, Lu D, et al. Influence of corneal topographic parameters in the decentration of orthokeratology. Eye Contact Lens 2019;45:372-6.
9) Mountford J, Cho P, Chui WS. Is fluorescein pattern analysis a valid method of assessing the accuracy of reverse geometry lenses for orthokeratology? Clin Exp Optom 2005;88:33-8.
10) Zhang L, Zhang Y, Liu Y, et al. A novel fitting algorithm for alignment curve radius estimation using corneal elevation data in orthokeratology lens trial. Cont Lens Anterior Eye 2017;40:401-7.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Download Citation
Download Citation Print
Print






