

ë ě´ě ěĽëšë íźëśęłźěě ë¤ěíę˛ íěŠëęł ěěźëŠ° 모ë°, ěěëłëł, 모ë°, íźëśíę´ëłëł, 돸ě ě ęą° ë° íźëśěŹě 몊ě ěźëĄ ěŁźëĄ ěŹěŠëë¤[1]. ě´ëŹí ë ě´ě ě ěęľŹę° ë
¸ěśë늴 ë§ë§ěěěźëĄ ě¸í ěę°ěĽě ę° ë°ěí ě ěěźëŠ°, ë ě´ě ě ę°ë ë° íěĽ, ë
¸ěś 기ę°ęłź ę°ě ěŹëŹ ěěě ë°ëź ë¤ěí ë§ë§ěěě ě ë°í ě ěë ę˛ěźëĄ ěë ¤ě ¸ ěë¤[2]. ë ě´ě ë
¸ěśëĄ ě¸í ë§ë§ěěěë ě¸ě¸Ąë§ë§íě´(outer retinal disruption), íŠë°ěśí(foveal hemorrhage), íŠë°ëśě˘
(macular edema), ë§ë§ě ë§(epiretinal membrane), ě 츾íŠë°ěęłľ(full thickness macular hole) ëąě íŹí¨íë¤[3].
ęšëšĄě ë°ěŹ ë° íě¤ë°ě(the blink reflex and aversion response)ě ë ě´ě ë
¸ěś ěę°ě 0.15-0.25ě´ëĄ ě íěí¤ë ěí ě íë¤. ꡸ëŹë ě´ëŹí ë°ěŹě ě¸ ëł´í¸ ëŠěť¤ëěŚě ěę°ě ě¸ ë
¸ěśěźě§ëźë ęł ěśë Ľ ë ě´ě ë
¸ěś ěěë ëší¨ě¨ě ě´ëŠ°, ěźěě ě¸ ë ě´ě ë
¸ěś íěë ěŹę°í ë§ë§ěěě´ ë°ěí ě ěë¤[4].
ęľë´ 돸íěě í´ëěŠ ë ě´ě íŹě¸í° ěĄ°ěŹ í ë°ěí ë§ë§ëłěŚ[5-7] ë° Nd:YAG ë ě´ě 뼟 ě´ěŠí íëě ę°ě ë° ě뼴곤ë ě´ě ę´ěęł ě ě´í ë°ěí ě´ě°¨ë§ë§ëłěŚě ëí ěŹëĄę° ëŞ ě°¨ëĄ ëł´ęł ë ë° ěěźë, 미ěŠěšëŁěŠ ęł ěśë Ľ Nd:YAG ë ě´ě ě ę´ěě ě°ě°í ë
¸ěśë ě´í ë°ěí ë§ë§ëłěŚě ëí´ěë ëł´ęł ë ë° ěë¤. ě´ě ě ěë¤ě 36ě¸ ěąě¸ěě 미ěŠěšëŁěŠ ęł ěśë Ľ Nd:YAG ë ě´ě ě ě°ě°í ë
¸ěśë ě´í ë°ěí ě¤ěŹě ë§ë§íěśíě ëí´ ííę´ë´íźěąěĽě¸ěí체(anti-vascular endothelial growth factor antibody)ëĄ ěĄ°ę¸° ěšëŁí ěŚëĄëĽź ëł´ęł íęł ě íë¤.
ěŚ ëĄ
36ě¸ě ěŹě íěę° ë´ě ěźěŁźěź ě 1,064 nm íěĽ 0.427 gigawatt (GW)ě 미ěŠěšëŁěŠ ęł ěśë Ľ Nd:YAG ë ě´ě ě ě°ě°í ë
¸ěśë ě´í ë°ěí ě°ěě ěë Ľě í뼟 죟ěëĄ ë´ěíěë¤. íěë ëšě ë ě´ě ěě ě ěí í
ě¤í¸ ęłźě ě¤ ě§ě ě ě¸ ë
¸ěśě´ ěë ě˘
ě´ě ë°ěŹë ę´ěě ěę°ě ěźëĄ ë
¸ěśëěë¤ęł ě§ě íěë¤.
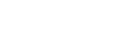
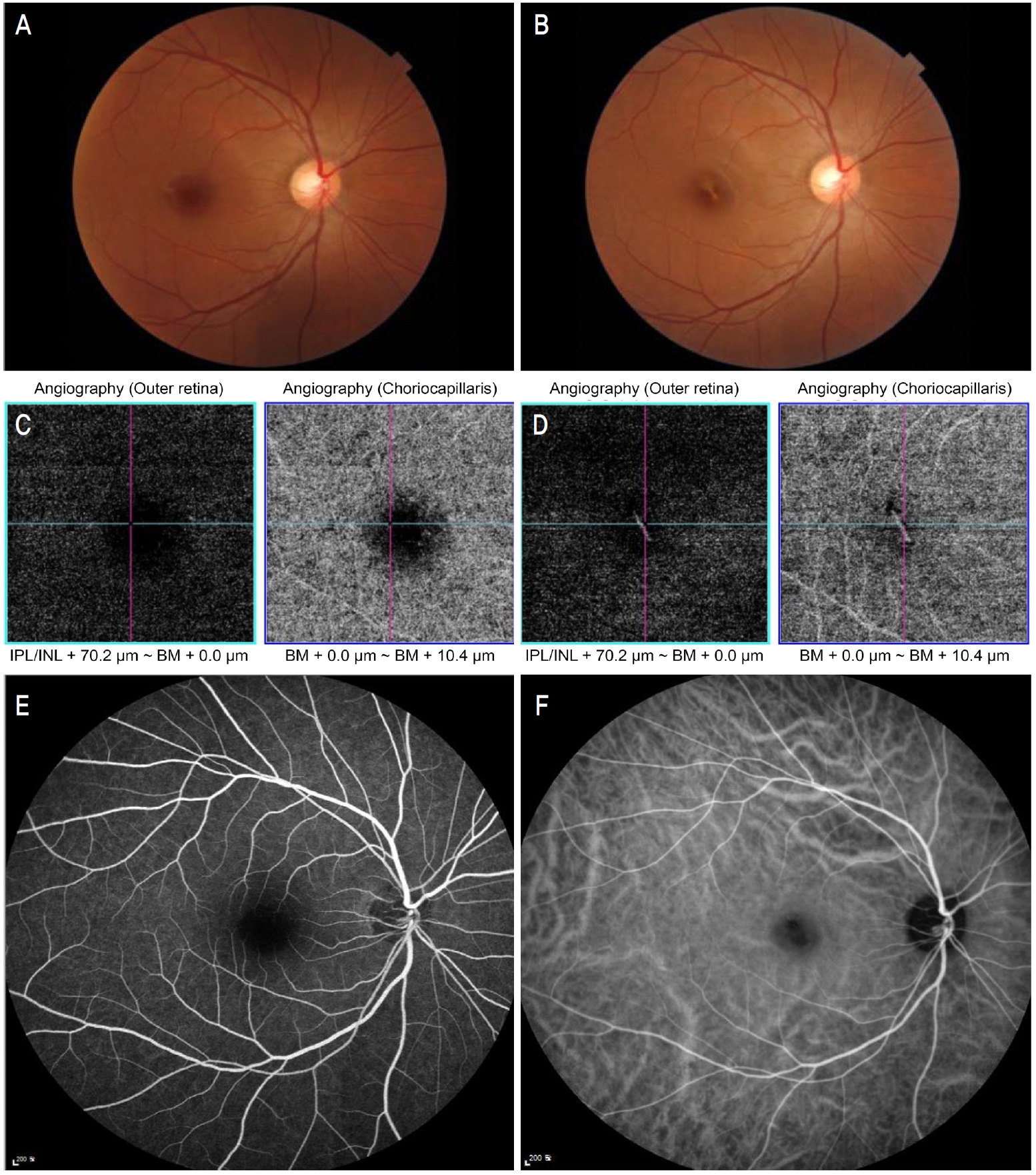
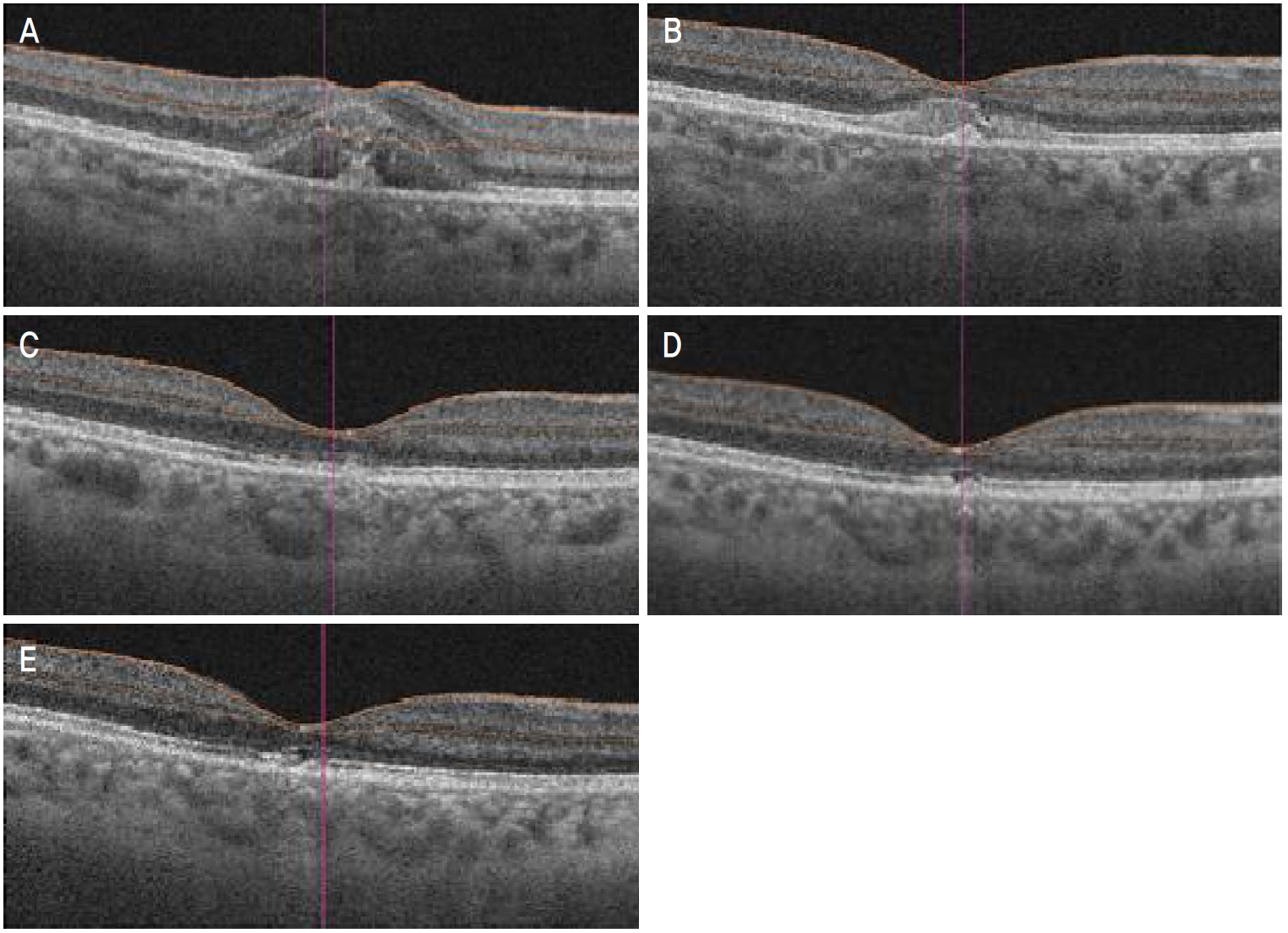
íě ęłźęą°ë Ľě ë´ęłźě ëłë Ľ ěěźëŠ°, ěęłźě ëłë Ľ ë° ěě ë Ľ ëí ěěěźëŠ°, ë´ě ëšě ěľëęľě ěë Ľě ě°ě 0.1, ě˘ě 1.0ě´ěęł , ëšě ě´ ěěęłëĄ 츥ě í ěěě ě°ě 16 mmHg, ě˘ě 13 mmHgěë¤. ě¸ęˇšëąí미경ę˛ěŹě 결ë§, ę°ë§, ě ë°Š, ëęłľ ë° ěě 체ë 모ë ě ěě´ěęł , ě°ëíěŹ ěíí ěě ę˛ěŹě ě°ěě 1ě ëě§ę˛˝ íŹę¸°ě ě¤ěŹě ë§ë§íěśíě´ ę´ě°°ëěë¤(Fig. 1A). ëšę°ěë¨ě¸ľě´Źě(optical coherence tomography)ěěë ě°ě ě¤ěŹě ë§ë§íěśíëĄ ě¸í ě ěěě ěĽěĄë§ë§ë°ëŚŹ ě겏 ë° ë§ë§ěěěíź-ë¸ëŁ¨íŹë§ íě´ëĄ ě¸í ěĽěĄë§ë§ë°ëŚŹ ě¤ěŹëśě ęł ěě ě겏ě ę´ě°°í ě ěěěźëŠ°(Fig. 2A), ëšę°ěë¨ě¸ľíę´ěĄ°ě(optical coherence tomography angiography)ěě ě¸ë§ë§ě¸ľęłź 맼ë˝ë§ëŻ¸ě¸íę´ě íëĽě íę° ę´ě°°ëěë¤(Fig. 1C). 맼ë˝ë§ě ěíę´ ě 돴뼟 íě¸í기 ěí´ íę´ěě íę´ěĄ°ěě (fluorescein angiography) ë° ě¸ëěŹě´ěë꡸댰íę´ěĄ°ěě (indocyanine green angiography)ě ěśę°ě ěźëĄ ěííěë¤. íę´ěě íę´ěĄ°ěěěë ë§ë§íěśíě ěí ě°ě ě¤ěŹě ě íę´ ě겏, ě¸ëěŹě´ěë꡸댰íę´ěĄ°ěěěë ë§ë§íěśíě ěí ě°ě ě¤ěŹě ě íę´ ě겏 ë° ě¤ěŹëśě ë§ë§ěěěíź-ë¸ëŁ¨íŹë§ íě´ëĄ ě¸í ě íę´ ěę˛Źě´ ëŻ¸ě¸íę˛ ę´ě°°ëěěźë ëë ˇí 맼ë˝ë§ě ěíę´ë§ě ę´ě°°ëě§ ěěë¤(Fig. 1E, F).
ě˛ě ë´ě í 1ę°ě, 2ę°ě, 3ę°ě, 6ę°ě째 경곟 ę´ě°° ěë§ë¤ ëšę°ěë¨ě¸ľě´Źě ë° ëšę°ěë¨ě¸ľíę´ěĄ°ěě ěííěŹ ě¤ěŹě ë§ë§íěśíě í¸ě ë° ěŹë° ěŹëś, 맼ë˝ë§ě ěíę´ě ě 돴뼟 íě¸íěěźëŠ° ě˛ě ë´ě ě, 1ę°ě, 2ę°ě째 ě´ ě¸ ë˛ě ęą¸ěł ě°ěě ě 댏체ę°ë´ ë˛ ë°ě죟ë§(AvastinÂŽ, 1.25 mg/0.05 mL; Roche Korea, Seoul, Korea) 죟ěŹě ě ěííěë¤. ě 댏체ę°ë´ ë˛ ë°ě죟ë§ěŁźěŹě ě ë ě°¨ëĄ ěí ě´í 2ę°ě째ëśí° ëšę°ěë¨ě¸ľě´Źěěě ě°ěě ě¤ěŹě ë§ë§íěśíě íĄě ě겏ě ëł´ěë¤(Fig. 2B). ěšëŁ ěě í 6ę°ě째 ěíí ěě ě´Źěěě ě¤ěŹě ë§ë§íěśíě ěě í íĄě ë° ě¤ěŹëśě ë°í ěę˛Źě´ ę´ě°°ëěěźëŠ°(Fig. 1B), ëšę°ěë¨ě¸ľíę´ěĄ°ěěě ě¸ë§ë§ě¸ľęłź 맼ë˝ë§ëŻ¸ě¸íę´ě íëĽë ę°ě ëěěźë ě¤ěŹëśě ë°í ěę˛Źě´ ę´ě°°ëěë¤(Fig. 1D). ë§ë§íěśíě ěŹë° ë° ë§Ľë˝ë§ě ěíę´ě 6ę°ěěŹ ę°ě 경곟 ę´ě°° ę¸°ę° ëě ë°ěíě§ ěěęł íě체꾏ě(ellipsoid zone) ë° ë§ë§ěěěíź-ë¸ëŁ¨íŹë§ ëłľíŠě˛´(retinal pigment epithelium-Bruchâs membrane complex)ě íě´ ě겏곟 í¨ęť 맼ë˝ë§ ë°í ěę˛Źě´ ëšę°ěë¨ě¸ľě´Źěěě ě§ěě ěźëĄ ę´ě°°ëěë¤(Fig. 2C-E). ěě 6ę°ě í ěľëęľě ěë Ľě 0.1ëĄ ě¸Ąě ëěë¤.
ęł ě°°
American National Standards Institute (ANSI)ě ë ě´ě 뼟 ěśë Ľě ë°ëź Class 1, 1M, 2, 2M, 3R, 3B, 4ëĄ ëśëĽíęł ěë¤. Class 3R ë ě´ě ě ę˛˝ě° 1-5 mW ěŹě´ě ěśë Ľě í´ëší늰 ANSI ě§ěš¨ě ë°ëź Class 3R ě´ěěěë ěë ¨ë ě´ěěě ę°ë
íě ěŹěŠíëëĄ ęśěĽíęł ěë¤[8]. Nd:YAG ë ě´ě ě ę˛˝ě° ěľë ěśë Ľě´ 100 mW ě´ěěźëĄ Class 3B ě´ěě ęł ěëě§ ë ě´ě ě í´ëšíëŻëĄ 죟ě ęšě ěŹěŠě ěíë¤. ę´ě ě 기본ě ě¸ ě¸ ę°ě§ 기ě ě¸ ę¸°ęłě , ě´, ę´ííě í¨ęłźëĄ ë§ë§ě ěěě ě¤ ě ěěźëŠ° ë ě´ě ě ěí ë§ë§ěěě 기ęłě , ě´ ěěě ěí´ ë§ë§ě¸ľě íę´´, ë§ë§ ë° ë§Ľë˝ë§ íę´ íě, ě§ě§ ęłźě°í ë°ěě´ ěźě´ë¨ěźëĄě¨ ë°ěíë¤ęł ěë ¤ě ¸ ěë¤[3]. ë ě´ě ě ěí ë§ë§ěěě 경꾏 ě¤í
ëĄě´ëě ë° íě°íě ę° íě°í ë° íěźěŚ í¨ęłźëĽź íľí´ íěĄ-ë§ë§ ěĽë˛˝ě ëł´ě íë ěí ě í¨ěźëĄě¨ ěšëŁě í¨ęłźę° ěě ę˛ěźëĄ ěę°ë늰, ě¤ě ëĄ ěë Ľę°ě ě´ ěěë¤ë ëŞëŞ ëł´ęł ę° ěěěźë ěë Ľěíě ę˛°ęłźę° ë¤ěíę˛ ëíëŹěźëŠ° íěŹ ěšëŁë˛ě´ ě 댽ëě´ ěě§ ěë¤[3,9-13].
ë ě´ě ě ěí´ ë§Ľë˝ë§íě´ě´ ë°ěíë ę˛˝ě° ě´ë ëë°ëë ë¸ëŁ¨íŹë§ íě´ě´ ë§ěą ěźěŚě ěźěźěź íę´ë´íźěąěĽě¸ě ëśëšëĽź ěíĽ ěĄ°ě í¨ěźëĄě¨ 맼ë˝ë§ě ěíę´ě ě ë°ěí¤ë ę˛ěźëĄ ěë ¤ě ¸ ěěźëŠ° 맼ë˝ë§íě´ íěě 10-20%ěě ë§ë§íěśí ë° ěĽěĄë§ë§ë°ëŚŹëĽź ëë°í 맼ë˝ë§ě ěíę´ě´ ë°ěíë ę˛ěźëĄ ëł´ęł ë ë° ěë¤[14]. 맼ë˝ë§ě ěíę´ě 맼ë˝ë§íě´ íěěě ěŹí ěë Ľěěě ěě¸ě´ ë ě ěë¤. Nd:YAG ë ě´ě ě ěí 맼ë˝ë§íě´ě ííę˛ ëł´ęł ëě§ ěěěźë ě¸ěěą ë§Ľë˝ë§íě´ íě뼟 ëěěźëĄ í ě°ęľŹěěë ěë Ľěíě ę´ë ¨ë ě¸ěę° ëł´ęł ë ë° ěëë°, Ament et al [15]ě 111ěě 맼ë˝ë§íě´ íě뼟 ëěěźëĄ í ííĽě ě°ęľŹěě ěë Ľěíě 맼ë˝ë§ě ěíę´ ë°ěě ě츥 ě¸ě뼟 ëł´ęł í ë° ěěźëŠ°, ě´ę¸° ěë Ľ ë° ěě ěěšę° ěë Ľěíě ě ěí ě°ę´ěąě ëł´ěěźëŠ° ęł ě°ë š ë° íŠë°ëś 맼ë˝ë§íě´ě´ 맼ë˝ë§ ě ěíę´ ë°ěęłź ę°í ě°ę´ěąě´ ěěěě ëł´ęł íěë¤. Liu et al [16]ěě íę´ë´íźěąěĽě¸ěě ěľě ë ěśí ěę° ë° ěęł ěę° ę°ě뼟 íľíěŹ ěśí íĄěěë í¨ęłźę° ěěě ëł´ęł íěë¤. ëí Kim et al [14]ě ě¸ěě ěí íŠë°ëś 맼ë˝ë§íě´ íěě ěë Ľě íě ěě´ ë§Ľë˝ë§ě ěíę´ ë°ě ě 쥰기 ë˛ ë°ěěŁźë§ ěŁźě
ě´ ë§ë§íěĄ ę°ě ë° ěë Ľí¸ě ě í¨ęłźě ě¸ ěšëŁëĄ ě ěí ë° ěë¤.
본 ěŚëĄěěë ě§ë¨ ě ëŞ
íí 맼ë˝ë§ě ěíę´ě ę´ě°°ëě§ ěěěźë ë§ë§íěśíě ěí ěŹí ěë Ľěěě ëł´ěë¤ë ě , ěě ëśěę° ě¤ěŹě뼟 íŹí¨í ě ě ęł ë ¤íěŹ ěśí 맼ë˝ë§ě ěíę´ ë°ěě ěíě´ ëë¤ęł íë¨íěěźëŠ° ě´ę¸° ěë Ľě´ 0.1ëĄ ě íëě´ ěě´ ěĄ°ę¸° ě 댏체ę°ë´ ë˛ ë°ě죟ë§(AvastinÂŽ, Roche) 죟ěŹě ě ěííěë¤. 첍 ë´ě í 2ę°ě째ëśí° ëšę°ěë¨ě¸ľě´Źě ë° ëšę°ěë¨ě¸ľíę´ě´Źěěěě ë ë ˇí ě°ě ě¤ěŹě ë§ë§íěśíě íĄě ě겏ě ëł´ěęł ë§ë§íěĄ íšě íŠë°íěśíě ěŹë° ě겏ě ę´ě°°ëě§ ěě ě 댏체ę°ë´ ë˛ ë°ěěŁźë§ ěŁźěŹě ě ěí í¨ęłźę° ěěěě ě ěśí´ ëłź ě ěěë¤.
íŠë°íěśí íĄě ě겏ěë ëśęľŹíęł ě¤ěŹě íě체꾏ě ë° ë§ë§ěěěíź-ë¸ëŁ¨íŹë§ ëłľíŠě˛´ě íě´ ě겏곟 í¨ęť 맼ë˝ë§ ěŹě¸ľëśě ë°í ě겏ě ě§ěëě´ ěë Ľě 0.1ëĄ ěśę° ę°ě ě ëł´ě´ě§ ěěë¤. ꡸ëŹë 본 ě°ęľŹë ęł ěśë Ľ 미ěŠë ě´ě ě ěí íŠë°ëś ěě ě ě 댏체ę°ë´ ë˛ ë°ě죟ë§ěŁźěŹě ě ě´ěŠíěŹ ě ěí íííě í¸ě ë° ë§Ľë˝ë§ě ěíę´ ë°ěě´ ěěěě íě¸íěë¤ë ě ěě í¨ęłźě ě¸ ěšëŁěě íě¸íěěźëŠ°, 본 íěë ě¤ěŹě 욨ë˛ě ěí´ ěë Ľěíë ě˘ě§ ěěěźë ě¤ěŹě ě¸ íŠë°ëś ěěě ę˛˝ě° ě 댏체ę°ë´ ë˛ ë°ě죟ë§ěŁźěŹě ě´ ěë Ľěíěë ëěě ě¤ ě ěě ę˛ěźëĄ ěŹëŁëë¤. ěśí 맼ë˝ë§íě´ íěěě ě 댏체ę°ë´ ë˛ ë°ě죟ë§ěŁźěŹě ě ěĽę¸°ě í¨ęłźě ëí´ěë ë§ě ěŚëĄëĽź íľí ě°ęľŹę° ë íěí ę˛ěźëĄ ěę°ëë¤.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






